Twitter, as everyone who uses it knows, is a cesspit: a place to get shouted at by strangers and fight off anonymous trolls. So imagine my surprise when my jokey little tweet set off an enormous wave of love, pride and the very best in humanity.
It was New Year’s Day. I was lying on the sofa with my 24-year-old son, Joey, and we were giggling at one of our routine jokes. I took a few selfies of us having a cuddle, was pleased with one of them and tweeted it out with the simple, ironic message: “So terrible being the dad of a learning-disabled young man.”
I thought nothing more of it until I returned to my phone and saw a steady stream of notifications: likes, comments and retweets.
Happy, ordinary things
I was especially struck by the hundreds of pictures pouring in of families with a learning-disabled relative doing happy, ordinary things – climbing mountains or walking on a beach, bouncing on trampolines and posing in Christmas pyjamas – all laughing, smiling and having infectious, glorious fun.
Each carried its own pithy little message of mock gloom: “Another day of misery”, “Awful sadness”, “Such dreadful hell” and so on. I replied to each one with mock sympathy: “Oh how awful”, “So grim”, “Thoughts and prayers”, and suchlike. For three frantic hours on Friday evening, I could hardly keep up. And, when I woke up on Saturday, it was still going strong. By Monday morning, I was on the Today programme on Radio 4 talking about what had happened and what I thought it meant. It was clear that Joey and I had struck a chord. Because families of learning-disabled children are so often made to feel that their situation is deeply tragic, my tweet, I believe, encouraged them to show that they don’t just love their child to the moon and back – their child has taught them more about life, love and laughter than outsiders might expect. And they wanted to express that publicly.
carried its own pithy little message of mock gloom: “Another day of misery”, “Awful sadness”, “Such dreadful hell” and so on. I replied to each one with mock sympathy: “Oh how awful”, “So grim”, “Thoughts and prayers”, and suchlike. For three frantic hours on Friday evening, I could hardly keep up. And, when I woke up on Saturday, it was still going strong. By Monday morning, I was on the Today programme on Radio 4 talking about what had happened and what I thought it meant. It was clear that Joey and I had struck a chord. Because families of learning-disabled children are so often made to feel that their situation is deeply tragic, my tweet, I believe, encouraged them to show that they don’t just love their child to the moon and back – their child has taught them more about life, love and laughter than outsiders might expect. And they wanted to express that publicly.
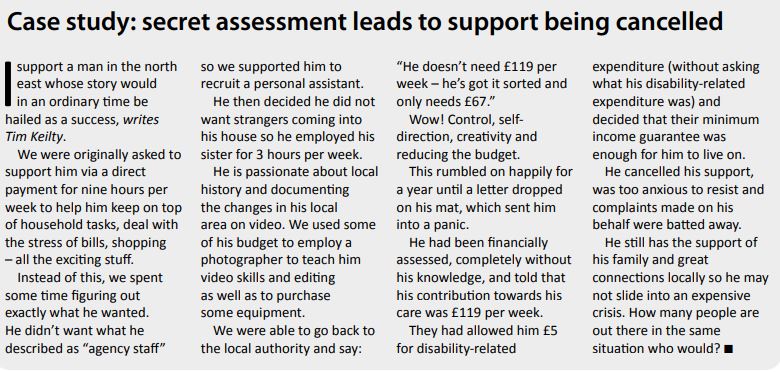
Joey, my second son, has severe learning disabilities and intractable (if medically managed) epilepsy. He has no speech and communicates with a limited vocabulary of simple Makaton signs, pointing fingers and a golden smile. He’s an endearing young man (I would say that, wouldn’t I?) who, for the most part, brings out the best in people. But he requires constant care to manage the simplest of tasks. His learning disabilities are not to be underestimated. When he was young, the suggestion was sometimes made that Joey must be a “sadness” to us. We constantly encountered tilted, concerned faces of – dare I say it? – somewhat manufactured sympathy, especially from people whose job it was to manage his future. In the process, we discovered that the only way to get him what he needed was to emphasise in the endless paperwork just how “bad” he was at everything – a failure and a danger to himself and others.
Parents revel in their children’s achievements, but those of us with learning-disabled children are forced to do the opposite – focus on the things they’re not good at and share, in crushing detail, our anxieties about their future. The struggle for Joey tore chunks out of us and such continuous negativity can be soul destroying.
Creative anarchy
What is forgotten is just how creative, enjoyable and splendidly anarchic sharing a life with a learning-disabled person can be. Joey has had a hugely positive impact on our family. I could not be prouder of the influence he has had on his elder brother, Laurie, and younger half-sister, Bea, who are much kinder, more intuitive and empathetic than I ever was in my youth. Clever as they are, they know that some things are more important than being brainy. Loving Joey is the easy bit. He’s no tragedy. It’s fighting for his future that hurts.
Parents of learning-disabled kids fight like Trojans to get our children what they deserve. But we’d gladly lay our weapons down if we could. We are driven by love –nothing else. There are challenges, frustrations and griefs to navigate. But raising a learning-disabled child really isn’t an unremitting tragedy. A particular mixture of pragmatic acceptance, raucous laughter and undying love rings through our houses.
This Twitter storm demonstrated that families don’t need “thoughts and prayers”. What we’re asking for is inclusion in all aspects of life and practical, high-quality and easily accessed support. Above all, we want society to embrace our kids as equals. As Joey’s then six-year-old sister once said to a friend alarmed by his lack of spoken language: “You don’t have to be scared of Joey. He’s just disabled.”
This life-affirming stream of beautiful photographs showed me that thousands of families with learning-disabled children are determined to bear witness to the unquenchable, overflowing love they feel for their children, however different, however ignored, however misunderstood. It’s just possible that the big-hearted and defiant response to my jokey little tweet suggests that things might change.
It’s a moment of hope.