Tracey Harding watches Kate Grant’s journey to becoming a model
True North: Role Model BBC 1, 11 June 2018
True North on BBC1 is a series of documentaries looking at life in Northern Ireland.
Each programme takes a 30-minute look at individuals or groups whose lives reflect the country’s diversity. Programmes have covered topics such as farming, tattooing after cancer surgery and a music festival.
This episode was dedicated to Kate Grant, a 19-year-old woman with Down’s syndrome, who wanted to be a model. It followed her attending a workshop for aspiring models, showing her on the catwalk of Belfast Fashion Week and modelling at a wedding fair (below and right).
Kate’s devoted family encouraged and supported her, and teachers at her school helped her transition into a college for people with learning disabilities.
In these respects, Kate was little different from others her age. However, the world of fashion and beauty can be impenetrable to anyone but particularly so for those with learning disabilities.
Kate trailblazing the way for other people with Down’s syndrome made her and her family incredibly proud. As her sister said: ‘Kate uses her disability as a voice to speak for those who can’t.’
The documentary portrayed Kate as an intelligent, determined young person who genuinely saw no barrier to achieving her dreams. It highlighted that there were no difficulties in employing a model with learning disabilities if the opportunities are available in the first place.
Kate really did look amazingly beautiful and confident on the catwalk, and the documentary was wonderfully inspiring to anyone of any ability thinking of taking the plunge into the modelling world.
As Kate’s father said: ‘If every parent and every family can develop each child to their full potential, how much more enriched our society could be.’
If you enjoy our free articles and would like to support our Campaigning magazine, providing legal articles on rights and good practice as well as comment on policy and practice concerns, why not SUBSCRIBE . You get a quarterly printed magazine & digital access to the archive and all current articles. Individual subs for a year start at £30 pa with concessions for students and unwaged carers
Vik JF finds unusual power in a striking exhibition that raises questions around complex collaboration and how an artist sees the world
In the beautiful gallery space of the Phoenix Brighton, I visited a really interesting and unique exhibition of the work of Johnny, who describes himself as an artist who is autistic.
Here was something I had not quite seen before – or at least I can’t remember that I have. In some of his works, Johnny paints only on the top three-quarters of the surface and creates a rounded border to separate from the white bottom, which felt so random and intentional at the same time (see photos below).
There was an interesting contrast between the vibrant colours and shapes and the bottom part that brings some calm balance to the work. Sometime drips run from the top part to the white and connect the two. If you turned the works upside down, they would look like mountains – the white part the sky, and the drips little stars. So, in a way it feels as if Johnny sees the world upside down sometimes.
Another theme I was curious about was the ‘man’, usually red on a blue background with very large hands – I was not sure if they are asking for help or about to attack. They reminded me of ‘Saturn devouring his child’ by Goya. These works feel very private.
My favourites were the black and white drawings. They look quick and spontaneous with lots of character – like a Picasso sketch. I could happily imagine them as a cool print on a t-shirt or in my living room. They have such happiness and rhythm with their rapid, upbeat lines.
The only thing that I felt that could have made this exhibition better would have been choosing less work and fewer themes. Johnny’s works are mostly very big and vibrant – they needed more space between them for people to experience the quality of each one.
That said, this was an incredible exhibition, put together by the Rocket Artists curation team. This is a group of 12 people, including Johnny and his parents, three artists from the Phoenix and six people from Rocket, who are artists with and without learning disabilities. It seems that this process was full of learning discussions and collaboration.
The exhibit I most enjoyed was the last room, where sticky tape in a variety of colours looked like a wonderful scribble across the whole space. It felt like a step beyond the clean, meticulously accurate tape installations I have seen before. It was free and messy in a charming way -a lovely representation of how complex a collaboration of this kind can be.
Art by Johnny, presented by Rocket Artists, was exhibited at Phoenix Brighton in April 2018
See more Art By Johnny at: http://tinyurl.com/yb8tfw48
Vik JF is an artist whose work mixes east and west, with English and Middle Eastern influences www.vikjf.com
If you enjoy our free articles and would like to support our Campaigning magazine, providing legal articles on rights and good practice as well as comment on policy and practice concerns, why not SUBSCRIBE . You get a quarterly printed magazine & digital access to the archive and all current articles. Individual subs for a year start at £30 pa with concessions for students and unwaged carers
Using film to bridge the parent-professional divide
Could film help parents and professionals to appreciate each other’s experiences and point of view? Clare Palmer, Henrik Lynggaard and Catherine Wordsworth discuss how films are being used to establish and sustain relationships
‘Working with challenging parents’ was a recent headline in an article for school staff in Tes on working with parents of children with special needs (Corby, 2018).
Not surprisingly, this caused much anger online among parents of children and adults with learning disabilities.
They responded in kind, asking: ‘How do you cope with challenging professionals?’
This illustrates just how quickly relationships between families and services can become polarised and how difficult it can be to establish and sustain collaborative working relationships.
In one of the training films we describe in this article, Owen Clinton, a family carer, observes:
‘This whole situation could be dealt with if family carers were regarded much more as a resource rather than something which had to be dealt with.’
We wanted to highlight and address some of the issues and dilemmas that can arise in the interactions between family carers and professionals. We developed two films and training resources entitled Learn With Us and Mind the Gap(s).
They were the result of a fruitful co-production between Family Carers in the London Borough of Islington, Islington Learning Disabilities Partnership and local charity Centre 404.
Family and professional carers
Learn With Us – Working in Partnership with Family Carers is a 45-minute documentary, beautifully made by Loaded Productions (www.loadedproductions.co.uk). It gives rare and remarkable insights into the experiences of family carers and staff who support people with learning disabilities.
Interviews with family carers, support workers and managers produce a thought-provoking narrative. The film opens with a moving poem by parent Jo Roach (see box).
Family carers discuss their intense anxiety about the future, especially over what will happen to their relatives with learning disabilities when they are not there.
Interviews show how the social model of disability applies to families, who share in the discrimination and disadvantage experienced by their relatives.
‘There were many things I would see a lot of my friends and their families doing, which, actually, we as a family could never do.’ Jignesh Patel, brother and family carer
The film emphasises that each family has its own back story, with difficult times. This theme is also echoed in staff comments:
‘Every family carer is individual in their approach, their response and their experience.’ Claire Curtis, housing manager
For my Daughter By Jo Roach
And you Suzie, what should I leave you?
Not the pewter statue of the boy
his right hand missing,
let him stay on the mantelpiece
for the second hand dealers.
Not photos of my mother who died
before you were born into that grieving time.
Not money, to be banked for you
by someone else.
Not my poems, you’ll never read them.
But the very fiercest of watchdogs
who wouldn’t sleep for a hundred years.
Published in “Oxford Poets 2007; An Anthology” by OUP and Carcanet Press.
The film includes two scenarios played by actors. In one, a mother calls the supported living house where her daughter lives to find out if she has gone swimming that day, as agreed in her review. This has not happened, and there is a major difference of opinion between the staff and the mother around issues of choice, confidentiality and best interest.
After the film was made, a three-hour workshop was designed and piloted with support staff. This includes group exercises and handouts. We wrote facilitators’ guidance for delivering the workshops. Family carers and managers work in pairs to run the sessions.
How to enable trust and good communication is a focus of the workshop, as is the importance of acknowledging and identifying the disagreement and moving forward, rather than avoiding problems and difficult situations. The film highlights how even small details can undermine trust and lead to a feeling of ‘what happens when I’m not here?’
Participants have given their views:
‘It filled a gap in my training I didn’t know existed till today.’ Support worker
‘I really enjoyed the day and came away feeling empowered and inspired. The people who appeared in the film were very brave and forthcoming.’ Family carer who attended a workshop sponsored by the National Valuing Families Forum
The sequel: an accurate portrayal
As with all good films, there was a demand for a sequel to Learn With Us.
Many people suggested we made another film, this time about the conflicts that can arise between family carers and social workers, and Mind The Gap(s) was born.
We all know there are excellent, dedicated staff who achieve good outcomes for the people they support and are much appreciated by families. We also know there are situations that are hostile, paralysing and exhausting for everyone involved.
People behave in ways that are deeply frustrating to others. They get labelled as The Problem – this could be the person with learning disabilities, family carer, social worker, manager or doctor.
We hear family carers say: ‘It’s not my disabled son/daughter who makes me ill – it’s dealing with the services.’
On the other hand, professionals will say: ‘There’s no problem with John/Mary – it’s their parents who are impossible/difficult.’
We worked with separate focus groups of family carers and professionals, asking them to discuss difficult experiences they had each had with the other.
Most evident were the Gap(s) in perceptions and feelings between the two groups. With the family carers, stories of anger, disappointment and grief dominated. With the professionals, what was most likely to emerge was frustration, questions of ‘Who is the client?’ and differing opinions about what was best for the person with learning disabilities.
The film, accompanied by a trainers’ resource pack, presents four situations of conflict or deadlock between a family with a son or daughter who has learning disabilities and the services working with them. In each scenario, actors play the parts of family members and social workers.
As well as illustrating disputes, we showed people speaking directly to camera as a way of demonstrating the underlying issues and emotions.
A unique feature of the film is the addition of two Gogglebox-style panels – one of family carers and the other of professionals – who comment on some of the issues raised.
The four scenarios that feature in the film are entitled Money, Transition, Review and Elderly Parents. They generate lively and wide-ranging discussion about the themes and dilemmas raised.
For example, in Review, an annual review is pending for Sarah, aged 30, who lives with her parents. She has learning disabilities with autism and some challenging behaviour. Her mother Anne is 55 and does voluntary work when she can. Her father Sam, 57, works full time.
The family have learned unofficially from a support worker that the social services department is planning that Sarah should attend a local day centre rather than the out of borough day centre she has attended for several years.
This decision is partly due to a policy of ‘bringing people back in to local services’ and partly on account of safeguarding concerns about the current day centre – which the new social worker is not at liberty to discuss as an investigation is under way.
Frustration turns to fury as Anne and Sam hear unofficially that their daughter is to be moved from the day centre she has attended for years – but social workers will not give all the reasons
The scenario starts with the parents calling the social worker in a worried and angry state, and Sam becomes increasingly enraged.
Mind the Gap(s) is accompanied by a facilitators’ resource pack, which can be used to run sessions of one, two or three hours.
We have been very pleased with the reception the film and the workshop have had. Professionals have said:
‘It is authentic and real. It reflects many of the situations we are dealing with in our everyday practice.’
Family carers have said:
‘This is a genuine portrayal of some of the difficulties we face.’
In our experience, the model of using films with training resources works well outside Islington, where other providers and councils are trying to improve partnership working with family carers.
The training workshops have offered a space for professionals, students and family carers where complex problems can be debated, giving participants a wider range of options for establishing collaborative partnerships.
For more information about the film-based training resources contact:
Clare Palmer, family carer, film producer, trainer: clarepalmer@yahoo.co.uk
Henrik Lynggaard, clinical psychologist, film producer, trainer: henrik3@me.com
Catherine Wordsworth, family liaison officer, Centre 404: catherinew@centre404.co.uk, www.centre404.org.uk/learnwithus
Corby G (2018) SEND: working with challenging parents. Tes, 22 May
If you enjoy our free articles and would like to support our Campaigning magazine, providing legal articles on rights and good practice as well as comment on policy and practice concerns, why not SUBSCRIBE . You get a quarterly printed magazine & digital access to the archive and current articles. Individual subs for a year start at £30 pa with concessions for students and unwaged carers Continue reading “Using film to bridge the parent-professional divide”
‘Contribution’ to statutory costs could be masking scale of funding cuts
How many of us could find an extra £60 per week out of our income – let alone at benefits level – with some extra essential expenditure because of disability?
My friend who acquired a brain injury in her late 40s/early 50s is supported on a direct payment (DP) which I manage for and with her. Because her short-term memory has been severely affected, she needs personal assistant (PA) support for day-to-day and a finance deputyship.
When I took on the DP role, we agreed a reduction in hours from 35 to 21 hours equivalent. The first financial assessment in 2015 was set at £57.64 per week. The council allocated £10 per week for disability related expenditure (DRE – extra costs due to disability) without ascertaining the real costs and we had to appeal to get it raised.
The appeal concerned DRE costs on extra heating, an annual holiday away (vital for wellbeing), house repairs, TV/phone, professional body membership, and dental and glasses charges; the allocation went up and the local authority charge was reduced to £17.28 per week.
Since my friend’s last assessment three years ago, her work pension has increased by only £20.49 per week. However, before we had any response to the appeal, we were told that the capped assessment at £60 was now to be £77.41. It took me three months’ chasing to get any contact and a reviewed assessment of £34.22.
Three months’ anxiety about the charge seems unacceptable. In addition, my friend is actually worse off as the financial assessment allows her to retain only the equivalent of a means-tested benefit. As she has a works pension, she is allowed none of the passported benefits (such as free prescriptions, dental and eye tests etc) for those on benefits only.
Fortunately, the replacement of disability living allowance with personal independence payment (PIP) increased her mobility rate to enhanced – this is disregarded in the care financial assessment rules – which should help her continued wellbeing in social activities with family and friends, including giving birthday and Christmas presents.
People deserve a life and not to be confined to home because there is no allowance for the costs of an active, contributing life, so unreasonable charge increases should be appealed. If costs are not in the support package, people should keep evidence of their spending.
In Control is running a survey to find about experiences about charges for care. This hidden ‘contribution’ by disabled people from their decreasing income towards statutory costs may be masking the real extent of the funding shortfall and will reduce independence and control. Please complete it so we can show what’s actually happening across the country.
The article on the Calderstones Hospital cemetery in our last issue (CL 31:4) stated that the bishop of Blackburn had rejected a request for partial deconsecration. In fact, the owners withdrew their application at the last minute.
They were unlikely to have succeeded, but withdrawal means they can re-apply.
The owners have recently submitted revised planning proposals to the council. These are opposed by the campaign group, as they still appear to pay scant regard to ashes interred in the Garden of Remembrance.
“Too often we buy mediocrity and push people into a half-life where their talents, hopes and potential are buried, when for less money we could enable them to be thriving citizens in vibrant communities.”
Our editor Simon Jarrett previews some of the articles in the latest issue of Community living and discusses the theme of transition – the changes that happen not just when someone reaches the age of 18, but all through their life.
For many years learning disability services, commissioners, and social workers have struggled to bridge the gap between childhood and adulthood – that moment when, usually at the age of eighteen, the transition takes place between children’s and adult services. Millions of pounds have been invested, there have been transition teams, joined-up service planning initiatives, specialist commissioning programmes and numerous ‘pilot’ projects that have sought the elusive holy grail of good practice in transition.
Why then, with all this attention, does transition still seem to represent an unfathomable divide in many areas, leading to real damage to the lives of many, who pass into inappropriate services at the age of eighteen and remain in them for the rest of their lives? In our current Autumn issue of the magazine (Community Living 32:1), we discuss the problems of child/adult transition in particular, and change generally, in the lives of people with learning disabilities.
There are specific problems about the transition to adult services that are well-known, such as failing to start the planning process early enough (ideally at age 14) and sometimes starting it catastrophically late (at age 17 ½). Many local commissioners and social workers still, too often, fail to involve families and the young person themselves in the process a meaningful way.
They do not seek creative local support networks that enable people to stay connected in their local areas, rather than be dispatched to high-cost, inappropriate, soul destroying institutional services in other parts of the country. Uncertainty about budgets often undermines planning and causes late, hasty, wrong decisions. Sometimes, incredibly, there is still not even reliable information held locally about who is going through the transition process.
But, as some of our writers in this issue highlight, there are deeper, underlying problems that undermine the change. Our columnist Simon Duffy of the Centre for Welfare Reform points out in his article ‘On the right road to adulthood’ that often a poverty of aspiration can pervade the whole process. We do not consider young people with learning disabilities as passing into a new life of employment, citizenship and opportunity, as we do with young people who do not have learning disabilities.
Instead, too often we seek services that will contain them, feed them, wash them and clothe them, and with luck offer them some activities to lighten the days. We often pay a lot of money to do this. We buy mediocrity and push people into a half-life where their talents, hopes and potential are buried, when for less money we could enable them to be thriving citizens in vibrant communities.
We know what needs to be done. We even know how it can be done. We now need the courage and aspiration to do it
Change is not just for your eighteenth birthday
The focus on transition at age 18 can mean that issues about change at other times in people’s lives are ignored. Once a young person is settled in their new ‘adult’ life, they can be left there for ever, as if no more change ever needs to occur. In another powerful article in this issue (‘To err is human, to live fully is divine’), Suzanne Gale asks ‘why do you only get one go at change when you’re an adult with a learning disability?’ People change throughout their lives. They change their ideas, they get in and out of relationships, they get married, become parents, and sometimes get divorced. They change interests, jobs and careers. They also get old, and eventually they die. All of these are natural transitions, but they are often not recognised in the lives of people with learning disabilities.
Like Peter Pan, they are expected to live a life of semi-childhood and arrested development – not their own, but imposed on them by society. Our articles on parenthood (‘To become a parent – and to keep your child’) and old age (‘Growing old the NICE way’) – show how we need to support people to embrace change throughout their lives. No one stops developing when they reach the age of 18, unless we stop them.
I hope you enjoy reading the articles in this issue – and if you want to join the debate about transition, let us know your thoughts – we’ll be very happy to hear from you.
If you enjoy our free articles and would like to support our Campaigning magazine, providing legal articles on rights and good practice as well as comment on policy and practice concerns, why not SUBSCRIBE . You get a quarterly printed magazine & digital access to the archive and all current articles. Individual subs for a year start at £30 pa with concessions for students and unwaged carers
In this article, Simon Jarrett, Community Living’s Editor and a Wellcome Trust Research Fellow traces the origins of some of the prejudicial ideas about the nature of learning disabilities through historical explorations of the supposed continuum of animals to humans.
In their quest to prove the interconnectedness of species, Victorian students of evolution viewed people with learning disabilities as proof of a human–animal continuum. Surprisingly, these ideas persist in some branches of moral philosophy today.
How did the minds of humans and other animals evolve from nothingness to consciousness? After Charles Darwin published his theory of evolution in 1859, scientists turned to the animal kingdom in their quest for answers. Somewhere in the evolutionary journey between the simplest single-cell organism and the higher primates, conscious thought must have emerged. But precisely at what point, and how did it come into being?
Our knees jerking when tapped is a reflex action. Comparative psychologists in the 19th century believed that ‘idiots’ were more reflexive and instinctive, and could be studied to help explain human evolution.
A new discipline of animal (or comparative) psychology was formed, which sought answers to the consciousness question by studying animal minds, from the most complex mammals to the lowest insects. Comparisons with the minds of human children and adults would, it was thought, throw light on the subject.
This intellectual endeavour was bad news for a certain type of human: those designated as ‘idiots’ at the time, broadly those we would categorise as having learning disabilities today. As the ‘lowest’ form of human mind, these people were compared – always unfavourably – with non-human animals.
Reflex, instinct and conscious action
A broad consensus was formed that consciousness evolved through a process that moved from reflex to instinct and then, in higher forms of life, conscious intentional action.
Reflex was the unthinking reaction of an organism to an external stimulus: for example, when our leg jerks upwards when our knee is tapped.
Instinct was a step up from reflex in the sense that whole species ‘learned’ reactions to stimuli – an eye closing when something comes too close – which were then acquired through adaptive evolution by future generations. Importantly, in this theory, instinct contained a limited amount of conscious action.
Full conscious action arose when individuals within a species learned to adapt their instinctive reactions to stimuli and situations they, or their forbears, had not encountered before. ‘Idiots’, regarded as the most reflexive and instinctive, and therefore least conscious of human beings, seemed an ideal object of study to demonstrate this theory.
In ‘Expression of the Emotions’ Darwin gave the example of joy and high spirits, which he saw as instinctive reactions across species to pleasurable feelings. “Idiots,” he claimed, “frequently laugh in a quite senseless manner” and would “grin, chuckle or giggle” when food was placed in front of them, or if they were caressed.
He argued that such reactions were nothing to do with ‘distinct ideas’ but were just instinctive expressions of pleasure. His theory was that joy or pleasure in the so-called ‘idiot’ was a bodily reaction to an external stimulation of the senses, like the way we cannot stop ourselves laughing when tickled.
Darwin considered joy an instinctive reaction that was easily aroused in ‘idiots’.
Darwin pointed out that the anthropoid apes (such as gorillas, chimpanzees and orangutans) were similar, and “utter a reiterated sound corresponding with our laughter when they are tickled, especially under the armpits”. (We should surely take our hats off to whichever Victorian gentleman of science first decided to tickle an anthropoid ape under the armpits!)
In ‘The Descent of Man’ Darwin made further ‘idiot’/animal comparisons when he claimed that ‘idiots’ were remarkably hairy, lacked speech, ascended stairs on all fours, climbed trees, smelled their food before eating it and made grimaces. He compared ‘idiots’ who were “continually gambolling about” with lambs, who “delight to frisk on any hillock”.
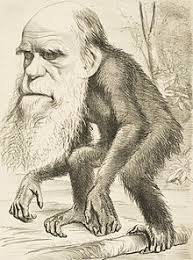
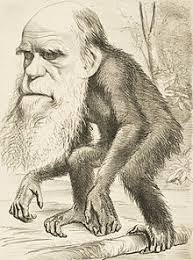
Darwin compared ‘idiots’ to apes. Often, those satirising Darwin’s ideas on evolution compared him to an ape in order to imply that he was idiotic.
Darwin hands on the baton
Towards the end of his life Darwin passed his uncompleted notes and manuscripts on instinct to a young protégé, George Romanes (1848–94). Romanes went on to write two volumes regarded as foundational texts for the discipline of animal or comparative psychology: ‘Mental Evolution in Animals’ (1883) and ‘Mental Evolution in Man’ (1888).
Romanes, a passionate Darwinian, was very keen to use ‘idiots’ to prove the evolutionary theory of mind. He claimed to have observed “primary instincts at work in startling ways in idiots” and described them as:
A class of persons… of peculiar interest in relation to mental evolution, because in them we have a human mind arrested in its development as well as deflected in its growth… supplying to the comparative psychologist very suggestive material to study.
He described visits to “idiot asylums” where he saw people carrying out “meaningless tricks of manner”, such as rocking, rhythmical movements and habitual gestures. He claimed that these were derived from hereditary instincts, which were once necessary but had outlived their use, and compared them to similar actions in dogs, cats and horses. Dogs turn around several times before lying down, he suggested, in an instinctive echo of their ancestors who lived in long grass and needed to trample it down before sitting.
Romanes believed that “useless” hereditary instincts characterised the behaviour of those people in the “idiot asylums” he visited.
Mind the consciousness gap
The use of idiots as ‘proof’ of the evolutionary development of mind by Romanes and subsequent comparative psychologists was extremely strategic. Their job was to explain the evolution of consciousness and the interconnectedness of species, both of which involved closing the consciousness gap between the human animal and other animal species.
If they could identify a type of ‘unevolved’ human whose combination of reflex, instinct and consciousness was close to non-humans, this could be presented as significant proof of the common descent of human and animal. The higher the levels of consciousness they could claim for some animals, and the more they could reduce the levels in some humans, the more the cross-species consciousness gap could be narrowed.
The IQ test is born
By the 1890s and early 1900s, the new concept of IQ (intelligence quotient) was being developed by psychologists in France and the United States. This suggested that a scientifically precise level of intelligence could be identified in any human, anywhere, through the application of a simple aptitude test. From this came the concept of ‘mental age’, which compared the mental functioning of a person to their chronological age.
Psychologists now considered themselves able to demonstrate ‘scientific’ proof of the comparative mental functioning of human infants, adult human ‘idiots’ and higher-functioning animals – particularly primates – through aptitude tests.
To this day psychology textbooks talk about the low ‘mental age’ of people with learning disabilities. Often the same age (usually somewhere between four and six) is attributed to primates who have taken similar tests, aimed at demonstrating their human-like capacities and consciousness.
Psychologists such as Edward Thorndike studied animals as well as humans in order to try to understand and measure intelligence.
The fallacy of the ‘bad’ human
The comparative study of animal and ‘idiot’ minds gave rise to new ways of thinking about the mentally incapacitated human that persist in contemporary society. A whole genre pervades our bookshops today, making claims about the abilities and consciousness levels of apes, monkeys, dogs, cats, birds, cows and even fish, which seek to narrow the consciousness gap between animals and humans.
Some philosophers, such as Peter Singer (author of ‘Animal Liberation’, 1975), claim that some non-human animals should enjoy greater rights than humans with learning disabilities.
The origins of these ideas lie in the work of Darwin’s disciple George Romanes and other late-19th-century animal psychologists. The Wellcome Library archives hold a superb collection of these works, which show how early animal psychology gave rise to a mode of thought about ‘good animals’ versus ‘bad humans’ that is very much with us today.
Simon Jarrett is a Wellcome Trust Research Fellow at Birkbeck University of London. He writes about the history of intellectual disability, human capacity and intelligence.
This report collated and shared the anonymised information about the deaths of people with learning disabilities so common themes, learning points and recommendations could be identified to be taken forward into policy and practice improvements. Many of these issues, and its recommendations, echo those of previous reports on the deaths of people with learning disabilities dating back more than a decade. It is more than 10 years since Mencap published Death by Indifference (2007) highlighting ‘institutional discrimination’ leading to the deaths of six people with learning disabilities whilst in the care of the NHS. Sir Jonathan Michael’s subsequent (2008) report ‘Healthcare for all’ expressed shock at the ‘disturbing’ findings of the inquiry, and concern that the experiences of the families described in Mencap’s report were by no means isolated.
The report found that people with learning disabilities died on average at age 58 yrs. Compared with the general population, the median age of death is 23 years younger for men and 29 years younger for women and often for entirely avoidable reasons.
The Government’s response begins with ‘Every death represents a deep personal loss to someone. How much more tragic is that loss when the person dies years earlier than expected, or as a result of something which might under different circumstances have been prevented? For people with a learning disability this is an all too common occurrence.The evidence of sustained and profound health inequalities for people with a learning disability is compelling and cannot be ignored.’
It has many expressed fine intentions, the question is will these be delivered in a timely way ir at all when we’ve seen so many more people die in circumstances which should have been prevented. Government response to the LeDeR report
We also believe that maybe this would not have got this far, had it not been for the painful but effective lobbying of parents – in particular #JusticeforLB and Dr Sara Ryan whose son died in the bath and who had to fight for 5 years to get an acknowledgement of the failures which meant hat this should not have happened.
Chris Hatton’s blog is a useful look at what this says and how it relates to the LeDeR recomendations – Valuing People then – the government response He ends by saying: ‘Including some things that are already happening makes sense (it would be worrying if there wasn’t anything already happening), but the inclusion of some actions that are not relevant, or working to timelines that don’t match each other, reduces my confidence that this scattershot approach will result in radical change.’ He asks ‘what are the elephants stalking this government response?’ Amongst these he notes the lack of analysis of what has gone wrong, no mention of the NHS 10 year plan which has identified learning disabilities as a priority nor any resources…..
Professor Chris Hatton is Professor of Public Health and Disability at the University of Lancaster whose research interests include examining and working to reduce the health and social inequalities experienced by people with intellectual disabilities. He is Co-Director of Improving Health and Lives (IHAL), the Public Health England sponsored Learning Disabilities Public Health Observatory.
Why was the so-called “idiot” population of Victorian Britain so important to Charles Darwin’s theory of evolution? Simon Jarrett looks back at a little-known aspect of his work that aimed to show there were close links between humans and animals
When Charles Darwin published On the Origin of Species by Means of Natural Selection in 1859, it is no exaggeration to say that he changed how we view the world.
He demonstrated that animal and plant species had slowly evolved over millions of years by a process known as natural selection, in which they adapted to their environment in order to survive.
Human beings and other animals had all begun as single-cell organisms in sludgy swamps, eventually becoming those marvellously sophisticated and complex organisms we are today.
This theory of evolution threw the world into disarray. It became difficult to maintain that human beings were specially created by God 5,000 years ago, as believed by those who interpreted the bible literally. The world was far older; human beings were much less special and of humbler origin than people had believed.
Many questions arose about human origins, and some were to have important implications for people with learning disabilities.
First, if humans and other animals evolved physically, they must also have evolved mentally. The human mind must have moved to full consciousness from a state of nothingness. How did this happen?
Second, if some human and animal species had the same origin, and if some animals evolved into humans, could we detect similar behaviours and mental activity across species to prove these connections?
“Lower” form of life
Darwin took a particular interest in those he called “idiots”, using the language of his time. He saw them as a “lower” form of human life; therefore, if he could show striking similarities between them and the “higher” animals, this would be evidence of the evolutionary process.
His aim was to narrow the consciousness gap between humans and animals, to prove that, while humans had developed into the most complex and sophisticated of all animals, they were far closer to animals both mentally and physically than people had been prepared to acknowledge. So-called idiots were, for Darwin, an excellent way of demonstrating this.
After Origin of Species, he published two books, The Descent of Man (1871) and The Expression of the Emotions in Man and Animals (1872). In both, he tackled the subject of human evolution.
In The Expression of the Emotions, he described joy and high spirits, which he saw as instinctive reactions across species to pleasurable feelings. He gave examples of “idiots” for whom laughter was the most prevalent emotional expression. This could not, he argued, be attributed to them having “distinct ideas” – they were just instinctive expressions of pleasure.
In The Descent of Man, he described what he believed to be the animal-like characteristics and habits of “idiots”, some of whom were “remarkably hairy”, lacked speech, ascended stairs on all fours, climbed trees, smelt their food before eating it or made grimaces. He compared those who were “continually gambolling and jumping about” with lambs who “delight to frisk on any hillock”.
These observations all supported Darwin’s emerging theory of how the mind evolved.
Intelligent life began with reflex actions, with no conscious thought or intention. Reflexes then developed into instincts, which involved a small element of consciousness, and were passed from generation to generation within species. Instinct then evolved into conscious action, in which animals, human or otherwise, could make choices as their minds developed memory and understanding.
Humans had the most highly developed consciousness of all, which is why reflex and instinctive actions were far less visible in them than in other species. Nevertheless, as observations of idiots, small children and higher animals showed, humans were built on reflex and instinct just like all the other species. Idiots were largely instinctive and reflexive, while “normal” infants developed into fully conscious humans.
Darwin’s theory gave rise to a new discipline of animal (or comparative) psychology. Practitioners observed animal behaviour and compared it that of to human infants and “idiots” to try to understand how the mind developed.
It was at around this time that the idea of “mental age” became important in psychology. Chimps could perform at the level of a four-year-old child when given tasks to do in experiments, seen as greatly to their credit. Adult idiots also performed at a similar level, much to their detriment.
This thinking persists today. Many books claim that apes, monkeys, dogs, cats, birds, cows and even fish are very similar in their mental lives to humans, and are conscious, intelligent and emotional beings.
Lurking beneath this school of thought lies Darwin’s quest to narrow the gap between the human and animal to prove evolutionary theory. A key element of that quest was to exaggerate the incapacities, inabilities and animal-like qualities of those he called idiots, to prove the animal-human link.
Darwin C (1859/1998) On the Origin of Species by Means of Natural Selection. Ware: Wordsworth Editions
Darwin C (1871/ 2004) The Descent of Man and Selection in Relation to Sex. London: Penguin
Darwin C (1872/ 2009) The Expression of the Emotions in Man and Animals. London: Penguin
Tracey Harding gives a round-up of the highlights and things to watch out for in the world of performance
Arts pioneers with learning disabilities are continuing to forge successful paths.
A taboo-breaking film continues to receive critical claim, Hollyoaks employs its first autistic actor and an underground performance has been showing some disturbing truths. Looking ahead, the First World War is to be interpreted in dance.
Enjoy some Sanctuary!
One of the films discussed in the previous issue of Community Living -Sanctuary by Len Collins – continues to be shown in film festivals around the world and garner praise and positive reviews.
This groundbreaking story of a couple’s overnight stay in a hotel helped to change the law in Ireland that made sex between learning disabled adults illegal.
The film is now more easily available for us all to enjoy as it has been released on digital formats. It can be found in the Sky Store, iTunes and Amazon so, if you haven’t managed to catch it yet, there really is no excuse.
Access All Areas: Madhouse Re: Exit and a new direction for Hollyoaks
An excellent theatre performance by a company of learning disabled and autistic actors is causing quite a stir.
Access all Areas production Madhouse Re: Exit enjoyed a sold-out run at Shoreditch Town Hall in London in March, before moving to Manchester as part of The Lowry’s Week 53 Festival in May.
It is reviewed in this issue by Sean Kelly (page 18) and discussed by Jan Walmsley (page 27).
The production is based on the story of Mabel Cooper, a resident of a long-stay hospital for people with learning disabilities who campaigned against these institutions. Five learning disabled actors stage an immersive underground journey, including audience participation, to portray the reality of what it feels like to be learning disabled in today’s society.
In an interview for The Stage, one of the performers – Cian Binchy, the autism consultant of the National Theatre’s The Curious Incident of the Dog in the Night-Time – spoke about the difficulties faced by actors with learning disabilities.
“The biggest challenge I face is that people with learning disabilities just aren’t seen as eligible to perform in theatres …. people with learning disabilities aren’t listened to …. We’re not given the opportunities. ”
“I first got involved professionally four years ago through Access All Areas’ performance-making diploma at the Royal Central School of Speech and Drama.”
The company, based in East London, offers innovative projects for people with a broad range of learning disabilities providing training in the arts. It also offers consultancy and training to organisations and employers, and has been an innovator in setting up the performance making diploma for learning disabled adults at the Royal Central School of Speech and Drama.
Soap’s new story
Access all Areas has also assisted with a groundbreaking first – it was involved in auditioning and casting for Channel 4 show Hollyoaks. It will be the first UK soap opera to feature a character with autism.
Talia Grant will be the first autistic woman to land a mainstream role on British TV. She was one of more than 150 applicants who auditioned for the role of school student Brooke Hathaway. Her character will feature in episodes from June onwards.
In addition to raising awareness of autism, it is encouraging to see TV script writers featuring autistic characters.
Magpie Dance
Magpie Dance, a company for people with learning disabilities is joining forces with Dr Lee Humber from Ruskin College, Oxford to research the effects of the First World War on people with learning disabilities.
The company, which is based in Bromley, Kent, aims to explore this history through dance.
Magpie says that research to date shows that, of the 40,000 people with learning disabilities housed in asylums across the country in the 20th century, up to 12,000 were displaced when the buildings were requisitioned as war hospitals. This led to overcrowding, insufficient staffing and consequently a disproportionately high mortality rate.
The partnership sounds like an amazing opportunity for a little-known part of learning disability history to be explored and presented to a wider audience. Fingers crossed for more great things in the future.
An online archive where people can share their stories about learning disability history has gone live, write Liz Tilley and Vicky Green.
The history of all kinds of people with learning disabilities in different circumstances is being brought to life in an online archive. This resource pulls together accounts concerning institutions, community services and advocacy – and more stories are sought
The Inclusive Archive of Learning Disability History (www.inclusivearchive.org) can be used by everyone, including people with profound and multiple disabilities.
The archive project ran over 2014-17. It built upon years of research supported by the Open University’s Social History of Learning Disability Group. It covers a wide array of work on the history of institutions, community services and advocacy bodies, much of which was generously financed by the Heritage Lottery Fund.
Twenty years after the group was founded, we decided it was time to pull together all the research, stories, memories and artefacts that people had collected.
We wanted to produce an online archive that would be fully accessible and enable people to make good decisions about what they shared, how and with whom. This meant building a team of researchers with and without learning disabilities who were employed as equals.
We also worked with local archives to explore how collections could be opened up to people with learning disabilities and what needed to happen to support more of them to participate in local heritage.
The aim was always to create an archive that was truly inclusive. So it needed to involve all people with learning disabilities – including those with profound and multiple learning disabilities, whose lives are so often hidden from public view.
To do this, we had to tackle confusion and anxiety regarding the Mental Capacity Act 2005 (England and Wales) and provide legal clarity around best interests decisions when it comes to sharing stories and depositing in archives. This was achieved.
In addition, the legal advice we secured has opened up opportunities to enable more people with learning disabilities to be involved in archives, which is a fantastic outcome.
Based on our research findings, we built a prototype, which is now live.
We would like to encourage as many people as possible to explore the archive and add their projects to it (see box). We are now developing the prototype into a sustainable archive to ensure all this wonderful material is preserved.
Find out about the project on its accessible website: http://inclusivearchiveproject.org
Vicky Green is a researcher and self-advocate; Liz Tilley is a lecturer at the Open University
Disability heritage backed by the lottery
Interested in how learning disabled people influenced everyday life in the past and today? Curious about how they change policy, influence activism and improve human rights for all of us?
At Heritage Lottery Fund, we are too, writes Liz Ellis. We use National Lottery players’ money to fund a wide range of activities that benefit heritage, people and communities across the UK.
HLF cares about inclusion. Since 1994, we have awarded more than £40 million to over 900 projects that specifically benefit disabled people, many of which enable them to explore the history and heritage of disability.
Our Inclusive Heritage conference in 2015, and popular Community Discussion Forum (see box) increase opportunities for people with disabilities to share knowledge about the projects they lead and boost expertise.
As a funder, we are always keen to promote great partnership and co-production models.
In particular, we are very proud to work with the Inclusive Archive Project, funded by the Arts and Humanities Research Council. We feel sure future HLF applicants will find inspiration in it.
Liz Ellis is policy adviser, community and diversity, at Heritage Lottery Fund
Asserting rights is not enough – what should we be fighting for? Jan Walmsley finds some inspired answers through creative, unconventional performances in mainstream arenas
I knew what I was fighting for once. In the mid 1980s, a time of fierce optimism, we knew what was right. Once we had closed the institutions and substituted an ordinary life, all would be well.
The certainty that state hostels, day centres and professional care were the solution was giving way to a more abstract clamour for rights. There was faith that self-advocates would forge a path, the need for support would somehow wither away and, after a period of dependence, people would manage their own affairs.
Looking back, it all seems idealistic – even naive – but this vision of the future provided inspiration and optimism.
While I’m sure that vision still inspires some, asserting rights can feel somewhat hollow when there are no means of upholding them in the face of government indifference or outright hostility. So, where else to look for inspiration?
Reflecting the articles about the arts in the last issue of Community Living, it is in the arts field where I’ve had my most positive and exciting encounters this year.
The first was as examiner of a wonderful PhD by Jade French (2018), a visiting research fellow at the University of Leeds. Her thesis was based on supporting five learning disabled people to curate an art installation at Liverpool’s Bluecoat Gallery – an amazing process and achievement.
The second was a musical performance in Watford by Electric Umbrella (electricumbrella.co.uk), a large, very diverse group of people with learning disabilities. It was probably the most inclusive event I’ve ever experienced. The music was exuberant and joyful, and everyone had a part if they wanted one.
The third was Access All Areas’ professional and challenging performance Madhouse Re: Exit (review, page 18).
I reflected on what these three had in common. Could they help me to put into words something to fight for?
Tracing the source
First, none sprang from service land. There was not a psychiatrist, psychologist, antipsychotic drug or support worker in sight. Those who funded, orchestrated and inspired the events were not people with learning disabilities or experts in the field. All three were led by individuals passionate about art, music or theatre who have found ways to share their passion with people with learning disabilities.
Second, all three gave “valued social roles” to those who took part. It is admirable to be a musician, perform in a professional theatre or curate an art installation in a prestigious public gallery. The events took place in mainstream not segregated settings.
What is so refreshing is that these roles were performed in far from conventional ways. I went round Madhouse with members of Blue Diamond, a group of people with Down’s syndrome who had come from Dublin to London to see it. Their response was visceral, energetic and energising. They talked back to the performers and cheered – they were doing it differently.
An audience member said to me afterwards: “I have no experience with disability, never spent time with disabled people – this makes me want to do it a lot more.”
Finally, they were fun, thought provoking, emotional and exciting in ways that mainstream art events often are not.
So what does this say about what I should be fighting for? To resist oppression, there are three broad strategies. One is to withdraw from society into a separate culture, such as L’Arche or Steiner villages. These communities suit some people well, and show alternative ways of living, defying pessimists and cynics and inspiring others.
The second is integration into the world as it is – broadly, the social inclusion approach. It requires a person to change to fit in as far as possible, to “pass” as normal and to adopt valued social roles. It is the most favoured current route – consider the emphasis on paid employment in Valuing People Now.
Finally, there is entering the world to change it – the most difficult as the world has to reconsider and adapt. The three events show attempts to do this by challenging what we think of as art and who does it; they provoke us to think differently about being an audience member or indeed a performer, and what it is to have a valued social role. Above all, they celebrate diversity by making it real.
It would be a better world if such experiences were common – and not just for people with learning disabilities. That has to be worth fighting for.
French J (2018) Art as Advocacy. Exploring Curatorial Practice by Learning Disabled Artists as a Tool for Self-Advocacy. www.fine-art.leeds.ac.uk/people/jade-french/
Large organisations are sweeping up tenders to provide advocacy services across the country. This is threatening grassroots projects that have grown over the years to meet the needs of individual communities, fears Peter Dawson
Advocacy started in the 1970s and 1980s for me, when I worked as a nurse for people with learning difficulties then as a service coordinator and training officer in social services.
I mistakenly thought at first that nurses and other caring personnel would be the most appropriate advocates for the people they looked after. Gradually, I realised that effective advocacy should be independent of services and based on clear, strong ideas of equality and citizenship.
Having been part of institutionalised care and knowing how disempowering it is, I felt strong support for the self-advocacy movement. From 1990, changing from service provider to advocacy enthusiast, I was able to work with colleagues with learning difficulties to develop self-advocacy groups in Derbyshire and elsewhere.
It seemed to me that groups should be as independent and self-managing as possible but also often need to be appreciated, understood and supported by people without disabilities to some degree.
Local voices
I had a role in the early days of Our Vision Our Future, which is still going strong in North East Derbyshire after 25 years. It manages itself, has not been hijacked or taken over by any other organisation and, despite funding cutbacks and other challenges, continues to grow.
It gives its members constant opportunities to develop self-confidence, skills, interests and a collective voice. They have always employed their own support and occasionally turn to trusted advisers outside their group for help. It is no thanks to me that they are still flourishing but, nevertheless, I am proud of that fact that, as someone without a learning difficulty, I am trusted to be consulted from time to time.
In the early 2000s, while working for Values Into Action’s advocacy project, I came into contact with many advocacy groups across the country. People First, based in London, is just one voice of people with learning difficulties; I cannot disagree with its strong commitment to the principle of “nothing about us without us”.
In 2004, I became manager of Peaks & Dales Advocacy, a small charity based in Buxton in the Derbyshire High Peak, an organisation that recognises the importance and centrality of self-advocacy.
We believe that good advocacy starts and ends with those we call our advocacy partners and what they want to say to other people who are usually in some sort of decision-making role, whoever they may be. The need for this sort of advocacy will end when society gets the message that everyone has worth and a right to a valued voice in their own lives.
For nearly 30 years, Peaks & Dales Advocacy has offered support to anyone in its area who needs it. These are not only people with learning difficulties but also those with mental health needs, older people and others – anyone who could be vulnerable to being ignored and marginalised.
Professional shift
However, I fear that much good, independent, locally based advocacy, which uses volunteer advocates and knows communities well, is being replaced by something different.
My own organisation lost its funding last year in a demanding, high-level tendering process. Now, one large organisation provides advocacy for everyone throughout Derbyshire.
Good luck to them and to the growing number of people who need and deserve advocacy support. I feel it will be hard for one major organisation to provide the locally sensitive, customised response that is so often needed.
This is a trend. Advocacy seems to be getting increasingly professionalised and “nationalised” – by which I mean there are large, national organisations sweeping up advocacy tenders throughout the country.
The best advocacy is consciously based on the principles of unconditional, positive regard promoted by Carl Rogers (1959). Like self-advocacy, it is a tool for empowerment.
Peaks & Dales Advocacy may have lost most of its funding for one-to-one advocacy but it still exists. We support a regular self-advocacy group who have recently made their own video and plan to produce more. We also are developing another tool towards empowerment – community development.
Many people in our area want meaningful things to do and opportunities to make and develop proper friendships and relationships of their choosing. For this, vulnerable people need information, communication and support to make and sustain informed choices. Maybe this is advocacy by another name Ð inclusion and equality continue to be our aims.
The work must go on. Our values have to be expressed in the way the work is done, not just in the outcomes – which is why the people we work with are our advocacy partners.
www.peaksanddalesadvocacy.org.uk
Peter Dawson is an advocate/senior advocacy development worker at Peaks & Dales Advocacy
Rogers CR (1959) A theory of therapy, personality, and interpersonal relationships as developed in the client-centered framework. In: Kirschenbaum H, Henderson V, eds (1989) The Carl Rogers Reader. Boston: Houghton Mifflin
Working together for better lives: Challenging ideas, passionate debate and vital information were generated at recent conferences
Legal and housing rights in a context of cuts
The hall was packed for Community Living’s eighth adult social care law seminar, Preventing Melt-down in Adult Social Care, held in March in Manchester, writes Rose Trustam. Belinda Schwehr, Community Living’s legal correspondent and founder of CASCAIDr legal charity, led the day with input from Mathieu Culverhouse from sponsors Irwin Mitchell solicitors.
Highlights
Key legal rights People should read the care and support statutory guidance so they can distinguish between duties and powers, shown in terms such as ‘must’, ‘expected’, ‘should’ and ‘may’ (https://tinyurl.com/care-sup-stat).
Can people get legal help? Mathieu Culverhouse of Irwin Mitchell Manchester said qualifying individuals (eg those who rely on benefits) can still get legal aid and cases can be brought by a litigation friend or family member. Crowdfunding to pay legal costs has been used by CASCAIDr.
Supported housing or residential care? The consequences of the Alternative Futures Group judgment in 2004, which said care homes could not be deregistered and turned into supported housing tenancies when personal care and accommodation were tied together, were discussed. Providers may put tenancies at risk and end up with a care home if they carry the cost of voids in shared supported housing rather than the local authority or company, or if the providers of accommodation and care are linked. People in shared supported housing could lose their entitlement to a personal budget if they have to buy care from the company that provides their home.
Budget cuts Statutory guidance says that, while a council can consider its finances when making decisions, it should not set arbitrary caps on costs and it should also choose the option that delivers the best value, not the cheapest option. How money is allocated should be transparent, rational and clearly explained before care planning starts; the amount needed cannot be cut just because of budget cuts.
Moving to save money People cannot be moved to save the council money because expecting them to leave a settled home would be a breach of their human rights. Whether they are living in a care home or supported housing, their human rights are engaged, and they have to be consulted and considered carefully, over and above any annual review or reassessment. If a person is mentally incapacitated, their best interests consultees must be involved, including the provider according to case law. A local authority would be in breach of its duty to promote an individual’s wellbeing if it did not assess this in each case.
Choosing a provider While there is no right to pick who provides support where this is commissioned, a person receiving a direct payment can choose any provider. They do not need to have full mental capacity to request a direct payment – knowing they want one and will need help with it should be enough. Most councils provide help to manage a DP as part of their wellbeing powers, although they do not have to. If an authority turns down a request for DP, it has to give its reasons.
Guides for people with learning difficulties and their families Irwin Mitchell has issued Meeting the Challenge – a good source of legal help, which includes advice for those stuck in assessment and treatment units. It can be downloaded from https://tinyurl.com/Irwin-meeting.
Tackling isolation, forging friendships and staying safe
Belonging was central to the North West Regional Self-Advocates’ annual conference in March in Blackpool, which had the theme What About Love, What About Trust, What About Us? writes Rose Trustam.
Highlights
Isolation Isolation was seen as a major consequence of service cuts. Lucy Hamlin from Lancashire’s U-Night group described how people can be lonely while surrounded by others, whether they are in a room, a house or a street. They need to know their assets and strengths and find connections in their choices.
Delegates wrote down what belonging meant to them. Only 3% of people with learning disabilities live with a partner (compared to 70% of the population). Six hundred and eighty people in the north west had addressed this in past two years; many formed friendships and one couple moved in together.
U-Night offer co-training (given by two people, one with a learning disability and one without) on dating, forging relationships and staying safe, which increases confidence.
Following U-Night’s lobbying, the Care Quality Commission now include questions about how relationships are supported when it carries out inspections.
Relationship support Kath Bromfield and Darren Hayward from Manchester People First spoke on their Small Sparks project. This provides small grants to help projects develop ideas to help people connect and build relationships. Hayward spoke passionately about the need for people to have control and a voice, as well as others in their lives to avoid isolation.
Learning Disability England held its inaugural conference, with the theme of the Challenge of Change, in Birmingham in December 2017, writes Jo Clare.
LDE had been launched only six months previously in June 2016, with the strapline Stronger, Louder, Together. It was founded by self-advocate Gary Bourler and Alicia Wood, former chief executive of the Housing and Support Alliance.
The event showed LDE had the hallmarks of an organisation that was still young and excited about its development and potential, but already coming of age and starting to realise its vision in the way that it did business
Karen Kirkpatrick, chief executive of Keyring and chair of LDE, asked in her conference address: “How can organisations back the ideas of people with learning disabilities without taking over?”
Answers came from models of good practice exemplified throughout the day – including a well-received presentation from Angela Catley from Community Catalysts – and the conference itself was a great advert for backing people without taking over.
Gary Bourlet looked at the extent to which people with learning disabilities were leaders, presenters and actors on the main stage at the event. He considered whether this matched LDE’s ambition for self-advocates to have a direct and authentic voice in and be at the centre of the movement for change.
This sense of voice was mirrored by lots of good-natured heckling, witty banter and spontaneous speaking out from people with learning disabilities; this demonstrated that, when self-advocacy is given the support, stage and status that it deserves, it can become infectious and spread.
Most of the day’s content, including sessions on supporting employment and staying safe online, flowed directly from the known concerns of people with learning difficulties and were correspondingly popular. Interest in the supported loving session, for example, was so great that people were hanging off door frames trying to get a look in.
At least as striking were the presence and leadership of family advocates, professionals and providers. They did not take over or pull strings from the gallery nor fall short of providing the advocacy, advice and information that is needed to support the challenge of change.
As well as insightful contributions from family carers such as Wendy Burt and Liz Wilson, there were invaluable presentations and sessions on subjects such as personal independence payments, funding for housing and sleep-in payments.
Professor Chris Hatton reported on what is happening to people in assessment and treatment units and inpatient services. For those who are still being detained and segregated inappropriately, as well as for those who are so disabled that self-advocacy is not possible, support from family carers with experience of this situation and advocacy by professionals and organisations are crucial.
If this conference is a mark of LDE’s intent, then at long last the sector has the potential for a united movement for social change – with people with learning disabilities at the centre, not the edges. LDE is not just one voice of learning disability but many voices and, so far, is promising to live up to its strapline, Stronger Louder Together.
Care assessment guide, capacity in religion and a call to listen to parents… Advocacy Focus celebrated 20 years of work with its Breaking Barriers conference in Preston in March, writes Rose Trustam
Highlights
Care assessments Advocacy Focus launched its Justice for LB toolkit, which was developed in consultation with Lancashire self-advocates. This gives professionals tools to help people with learning difficulties become more involved with their care assessments; it also provides information and guidelines about working with people who have learning disabilities or communication or cognitive issues. Download the toolkit from: www.advocacyfocus.org.uk/justiceforlb.
Capacity A barrister led a workshop that examined a court of protection case about religious observance (IH (Observance of Muslim Practice) [2017] EWCOP 9). Should religious practices of removing body hair and fasting be followed with a young Muslim man with no speech and a history of challenging behaviour?
The court ruled, with intervention from a psychiatrist and a cultural expert, that neither the fasting nor the hair removal were necessary or in his best interests. However, it was right that he should join in Eid and family celebrations, which he enjoyed.
The cultural expert clarified that, as the young man did not have legal competence, there was no obligation to carry out religious rites and that he would be seen as being in a perpetually heightened state of spirituality (a comfort to the parents).
The case showed that where there is anxiety about racism or discrimination, resolution can be reached by following the Mental Capacity Act and acting in the person’s best interests.
Combining health and social care services makes sense on the surface, but they have different objectives and priorities, argues Robin Jackson. He suggests that, to avert the looming crisis, we need to create a model that concentrates on social care rather than rely on merger
Social care is in crisis and, without radical changes in the very near future, I believe it will collapse.
Reforms introduced by successive governments have left it seriously underfunded and underperforming. It has become heavily dependent on the profit-oriented private sector and outsourced provision by powerful global companies which have frequently been exposed as incompetent and, on occasions, criminally irresponsible.
Many for-profit companies providing care have shown scant interest in maintaining adequately staffed facilities and an appropriately trained workforce. Companies have a strong incentive to keep running costs down by employing poorly qualified staff and maintaining less than full staff establishments.
This crisis will be made worse by merging health and social care.
The idea of merger appears to have arisen from the belief that the benefits of the two sectors are greater when they are combined into one rather than left as separate entities.
However, this is mistakenly built on the assumption that there are strong similarities between health and social care.
Why synergy fails
There is a belief that synergy inevitably confers advantages. However, it frequently fails because those seeking it focus too much on the financial and strategic aspects of merging and frequently underestimate the cultural aspects of the organisations being brought together.
In the one sector that one might reasonably have expected synergy to have a successful track record – mergers and acquisitions in banking – Leon Cooperman, a former Goldman Sachs partner, has confessed to being unable to identify one example where a merger has succeeded.
Defining the difference
The National Framework for NHS Continuing Healthcare has attempted to clarify the difference between healthcare need and social care need.
While there is no legal definition of a healthcare need, in general terms, it can be said that it is related to the treatment, control or prevention of a disease, illness, injury or disability, and the care or aftercare of a person with these needs, regardless of whether the tasks involved are carried out by a health professional.
In general terms – again, there is no legal definition – a social care need is one focused on providing assistance with activities of daily living, maintaining independence, social interaction, enabling the individual to play a fuller part in society, protecting them when their circumstances make them vulnerable, helping them to manage complex relationships and, in some circumstances, accessing a care home or other type of supported accommodation.
Social care needs are directly related to the type of welfare services that local authorities have a duty or power to provide. These include but are not limited to: social work services; advice; support; practical assistance in the home; assistance with equipment and home adaptations; visiting and sitting services; provision of meals; facilities for occupational, social, cultural and recreational activities outside the home; assistance to use educational facilities; and help to find accommodation such as a care home.
The essential characteristics of social care have been identified (Williams, 2003).
First, care of both the self and others are meaningful activities in their own right; they involve us all, men and women, old and young, able bodied and disabled. Therefore, care is an activity that binds all.
Second, in receiving and giving care, we can, in the right conditions of mutual respect and material support, learn the civic virtues of responsibility, trust, tolerance for human limitations and frailties, and acceptance of diversity.
Third, an ethic of care demands that interdependence be seen as the basis of human interaction; in these terms, autonomy and independence are about the capacity for self-determination rather than an expectation of individual self-sufficiency.
Fourth, it attributes moral worth to key positive dimensions of caring relationships such as dignity and the quality of human interaction, whether based upon blood, kinship, sexual intimacy, friendship, collegiality, contract or service; it recognises and respects diversity and plurality in the social process of care.
Finally, it argues against inequalities in the giving and receipt of care. It recognises these inequalities may be constituted through different characteristics, including sex, disability, age, ethnic origin, nationality, class and occupational status, sexuality, religion and marital status.
Care requires time, financial and practical support and the recognition
of choices. These extend beyond income maintenance, benefits and social services to include public space, transport and policies to address discrimination and poverty.
A department of social care?
To prevent a collapse of the social care system, I would argue for the creation of a single government department responsible for just social care.
Such a department would establish the principles and guidelines for social care. Furthermore, the operation of the system would be devolved to regional councils in a system comparable to that in Sweden, which existed in the UK before 1974. It’s worth noting that reorganisation in 1974 was intended to reduce the amount of money spent on public services and to ensure increased efficiency, neither of which was achieved.
The establishment of a central government department of social care can happen only if sufficient financial resources are made available. In my opinion, the best option would be to increase income tax in a discriminating manner – as in Scandinavia Ð or to introduce a social care tax. The UK is behind the overwhelming majority of western European countries in the amount allocated to social expenditure; it was the only rich EU country to cut welfare spending as a proportion of GDP between 2011 and 2014.
A strong case has been made by for introducing a hypothecated tax where the revenues from the tax go to financing a particular service such as social care (Keable-Elliott, 2014). This approach has a number of advantages:
Transparency – hypothecated taxation makes the link between revenues from taxes and government spending more visible
Accountability and trust – hypothecated taxes may help when the government is not trusted. With hypothecation, the government will have to follow a plan made in advance and will have no flexibility
Public support – the knowledge that the money paid on taxes will go directly to some needed service (social care) can help to reduce the dissatisfaction of the population with an increase in taxes
Protecting resources – earmarking can protect resources for financing social care from being spent on something else.
If taxpayers are aware that a dedicated amount is set aside to fund a particular service, such as social care, there is a high probability that they will be supportive of such a measure.
It would be incumbent upon the government to demonstrate that the hypothecated tax was being used for the purposes agreed.
Collapse and its consequences
Unless major reforms of the kind very briefly touched upon here are implemented, there is a high probability that social care in England will collapse.
The consequences of that for the social fabric of the country will be disastrous. For a society already characterised by increasingly sharp social divisions, the loss of an effective social care system to support the disadvantaged could well prompt civil unrest and disorder.
The problem has been that successive governments of all political persuasions have misguidedly placed their faith in solving problems by attempting macro solutions, none of which have worked.
If a genuinely caring society is to be created, then we need to seek micro solutions which foster localism and community endeavour and enable people to truly take back control of their lives.
If such action is not taken, there is a strong probability that an Americanised health and social care system will emerge, which fails the overwhelming majority of the population but has minimal impact on the moneyed few.
The kind of reforms briefly touched on here are unlikely to be brought about by any of the major political parties. However, as a result of the fractious and fracturing pressures within the different political parties over Brexit, we may see the emergence of a new progressive political alliance with a radical and strong community-oriented agenda. There is then a glimmer of hope.
People with learning disabilities may experience depression for longer than other people. Chris Hatton worked on a study led by Andrew Jahoda to examine the effects of adapted versions of psychological therapies and whether they should be offered
Key messages
Adults with learning disabilities who are depressed can be helped by adapted versions of psychological therapies that are routinely offered to everyone else.
Psychological therapies can reduce anxiety and help improve the quality of life of adults with learning disabilities who are depressed. These therapies are not expensive and can be delivered to a high standard by community learning disability nurses and a wide range of other professionals, with some training and supervision.
Adapted psychological therapies should be made routinely available to people with learning disabilities and mental health problems.
Background
People with learning disabilities are at least as likely as other people to experience depression; their depression is more likely to be enduring, possibly because it is more likely to go unrecognised.
The National Institute for Health and Care Excellence has issued guidelines on how to help people with learning disabilities and mental health problems (NICE, 2016).
Therapies or psychological interventions, such as cognitive behaviour therapy, behavioural activation and guided self-help, are all recommended for helping people with depression in these guidelines. However, NICE found that there was little evidence about whether adapted versions of these therapies were useful for people with learning disabilities who are depressed.
This research project used a gold standard method Ð the randomised controlled trial (RCT) Ð to compare behavioural activation and guided self-help in people with learning disabilities who are depressed.
Methods One hundred and sixty-one adults with learning disabilities from Scotland, North Wales and North West England who had been diagnosed by the project team as depressed took part in the project. Everyone gave their consent to take part, and had a supporter who knew them well with them in the therapy sessions.
All participants received help; it was randomly decided who would receive behavioural activation and who would get guided self-help. Behavioural activation involved 12 sessions with a trained therapist to help the person take part in more activities and work through any barriers getting in the way. Guided self-help involved eight sessions with a trained therapist working through four booklets focusing on major issues in depression, such sleep and problem solving. Therapists were mainly community learning disability nurses.
Information was collected from participants at three points: before the therapy started; four months afterwards (when the therapy would have finished); and another eight months after that (12 months from the start). Everyone was asked about their depression and other aspects of their life, including what health and social care services they were using.
Findings
Behavioural activation and guided self-help resulted in people both becoming substantially less depressed by the end of their therapy sessions, and staying less depressed eight months after the end of the therapy. This was the same for anxiety, which was reduced and stayed lower.
Quality of life improved over the course of both therapies; this was sustained eight months after the end of therapy.
There were no important differences between behavioural activation and guided self-help Ð both had a positive effect.
Carers also reported their confidence in helping people with emotional difficulties had improved by the end of the therapy sessions; this had not changed eight months afterwards.
Behavioural activation, because it lasted longer, was more expensive (average £1,789 per person) than guided self-help (average £1,019 per person). Relatively speaking, both ways of helping people were not costly given that people were on average using health and social care support costing well over £20,000 per year per person.
Views gathered through in-depth interviews with some of the participants with learning disabilities, their supporters and the therapists showed that almost everyone found the adapted therapies engaging and helpful.
Supporters were generally felt to be useful both in and between the therapy sessions, although social isolation made it hard for some people to find a consistent, reliable supporter.
Audio recordings of a selection of therapy sessions showed that those delivering the therapies, mainly learning disability nurses with little or no experience of doing any therapy work, were providing each therapy to a high standard.
Conclusions
The types of therapies or psychological interventions that are helpful for depressed people generally can be adapted to work just as well for people with learning disabilities.
They can make a difference to both peopleÕs depression and to their lives more generally.
The therapy is not expensive, and can be delivered and done well by community learning disability nurses as long as they are trained and supervised.
There is every reason to make these and similar ways of helping people with learning disabilities and mental health problems much more widely available.
Comparison of behavioural activation with guided self-help for treatment of depression in adults with intellectual disabilities: a randomised controlled trial
Aims To compare two ways of helping people with learning disabilities who are depressed – are they helpful in reducing people’s depression and improving people’s lives more generally, and how much do they cost?
Methods A group of 161 adults with learning disabilities and a diagnosis of depression were randomly assigned to receive behavioural activation or guided self-help. Therapists were mainly community learning disability nurses. People were asked about their depression and other aspects of their lives before the therapy started, four months after the start (when the therapy had finished) and one year from the start.
Results and conclusion Both methods improved quality of life and reduced depression, and continued to do so a year after the project started. The therapies are not expensive and can be done well by community learning disability nurses.
Read the report Jahoda et al (2017) Comparison of behavioural activation with guided self-help for treatment of depression in adults with intellectual disabilities: a randomised controlled trial. The Lancet Psychiatry; 4(12): 909Ð919. https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(17)30426-1/
This project was led by Andrew Jahoda at the University of Glasgow.
National Institute for Health and Care Excellence. NICE Guideline NG54: Mental Health Problems In People with Learning Disabilities: Prevention, Assessment and Management. London: NICE. www.nice.org.uk/ng54
A light was shone on the stories and legacies of institutions at an exhibition about Calderstones and Brockhall hospitals. David O’Driscoll viewed some service history
“You’d Hear Them Jingle.” Views of Institutional Life. Voices from Brockhall and Calderstones, Clitheroe Castle Museum, Lancashire
Few of my colleagues working in learning disabilities today have experience of the long-stay hospitals that once dominated our services.
As a Hertfordshire NHS history project worker, I once made an unsuccessful attempt to develop an exhibition on the history of three local institutions (CL 30:3 2017). So when I heard about an exhibition on long-stay hospitals – You’d Hear Them Jingle – I knew I had to see it.
The title refers to a remark made by a former patient about staff coming down the corridor with their keys.
The exhibition examined the history of two long-stay hospitals, Brockhall and Calderstones, which were a few miles apart. Both opened after the First World War and closed in the 1990s. Both were major institutions holding up to 2,000 patients.
The exhibition featured oral history by family members, patients and staff. Memorabilia included nurses’ uniforms, patient menus and, of course, keys. There was also a short film, made in 1968, about Brockhall patient Bill Howe (view it at www.youtube.com/watch?v=LRFskr_5vHI).
Views on the hospitals contrasted. One nurse recalled: “I think the staff, the artisan staff, and the drivers and the laundry, they all cared about the staff and patients alike. Everybody cared somehow.”
However, another, who worked there in the 1960s, said: “They were rough tough places, institutions. I can’t hand on heart say I’ve ever seen any extreme cruelty – which I think is a tribute to the place given the times – but it was hard. It was a hard, hard place, and it sort of made you a bit hard as well, as time went by.
“You recognised how [staff] became institutionalised themselves …. they fit into this very cosy and pleasant place to work.”
One resident said: “They used to give you Largactil [chlorpromazine] syrup … to quieten and calm you down. It had a nasty, sweet taste. You got it for shouting and arguing. It made you go to sleep – dopey.”
Dr Nigel Ingham developed the exhibition with the help of Professor Duncan Mitchell. It was part of a project by Pathways Associates, supported by the Heritage Lottery Fund, to develop a digital archive: www.lancs learning disability institutions.org.uk/
Everyone needs meaningful relationships. Sue Deeley and Julie Smith tell the stories of two people that Getta Life has supported
Vicki Norton likes to be around children and talks easily with them. Four years ago, she went to help out at a stay and play group.
Staff have spoken about her contribution and how she has changed their thinking. Originally, they thought it would be something that only she would benefit from. Now, they recognise what she brings to the group. She has developed strong relationships with the children.
One boy who had always been lively and active became much calmer and talked with her through playing with playdough and Lego. When old enough for school, he invited her to his childminder’s home for a leaving party.
It was notable how many children and adults made a specific effort to find Norton and say goodbye at the end of sessions. Adults appreciated the opportunity for both their children and themselves to chat with a person with disability.
She became a part of the volunteer social group, attending coffee get-togethers and Christmas meals out.
Sheila Spicer has a wide circle of friends, all of whom met through her and are now deeply connected. These loving friendships have transformed how she sees herself – is perceived by others.
Spicer was sent to live in an institution when she was two years old. She left almost 50 years later. When we first met her, she sat with her head down, rocking, often crying and obviously very sad.
There was no one in her life who had not been paid to be there.
Slowly, things began to shift – having her own home, shared with two people she chose, gave her certainty. Support from a small, consistent team of people who wanted to know her helped her to trust.
Spicer began to show us herself. She is warm, funny, dignified and very gentle. She began reaching out.
We began to think about how we could help her to become known outside her staff team. Two people were asked if they would like to get to know her and the first two friendships in her life were formed. With support, she hosted lunches. The friends went out for afternoon tea, visited the theatre and shared birthday and Christmas celebrations.
While Spicer showed her appreciation of her new friends through gestures and smiles, the friends started to talk about what she was offering them – such as a chance to get together to share experiences and hang out over good food.
New people joined the circle and she now has at least six friends. They keep in touch individually and meet as a group. The times when they meet up are remarkable – there is so much love, great stories, lots of fun and deep concern for each other. Spicer supports her friends. She has her own car and helps them to go shopping and attend hospital appointments, and travels to see one friend who has moved away.
Below are comments by her friends:
“I am so proud to know Sheila – my life has changed completely. I have made a whole new group of friends from knowing her.”
“If you had told me I would be friends with someone who didn’t talk, I would say ‘how?’ as I talk a lot. However, Sheila has a lot to say and I get a lot from being Sheila’s friend.”
“It’s the friendship that matters most.”
Staff help Spicer plan how to meet her friends and keep in touch with each other. Their role is to support her to be a friend – not to make friendships for her.
Sue Deeley and Julie Smith are founders and directors of Getta Life
Getta Life believes that people with severe learning disabilities should be able to live their lives in their own homes with support to realise their dreams.
This small Coventry-based organisation’s work is built on the principle that everyone needs meaningful relationships, everyone can say what they want if people hear them and inclusion in all parts of society is everyone’s right.
Finding our role and our contribution to the world is a big part of how we discover who we are. For people who need support, the importance of this is often overlooked. To change this, we need to ask: what are their gifts? What brings out the best in a person? And how do we help someone gain more experiences that draw on these?
Working with people’s gifts, supporting them to find their purpose and build and nurture relationships is a conscious part of our work. Support staff must think deeply about those they support, and their role in developing a culture of community and belonging. www.gettalifeonline.co.uk
An immersive performance raises uncomfortable questions over the status of people with learning disabilities in society. Have dated attitudes really been consigned to history? asks Seán Kelly
“I’m shell shocked!” said an audience member at the end of the immersive theatre show Madhouse Re: Exit performed by Access All Areas at Shoreditch Old Town Hall in London earlier this year.
A group of us had spent the afternoon stumbling through dusty and sometimes smoke-filled corridors into rooms where actors took part in interactive scenes.
The show was based partly on the life story of Mabel Cooper in St Lawrence’s Hospital in Surrey, which closed in 1994 after over 100 years as an asylum for people with learning disabilities.
In the show, we saw a patient being assaulted by a member of staff and learnt about some of the degrading aspects of institutional life.
Five lead performers with learning disabilities took their cultural references from a wider arena. David Munns played Patient 36, a subversive virtual guide appearing on screens or as a holograph. Imogen Roberts’ character was inspired by the ancient Olmec civilisation in Mexico, where people worshipped those with Down’s syndrome, believing them to be related to jaguars. She performed a remarkable dance before declaring herself a jaguar goddess.
Cian Binchy played an infantilised adult, complete with a huge baby suit and cot. When the carer took his nappy off, she discovered a large rubber penis, which she removed. The character complained: “You think it’s creepy that we actually have sex because you think we are children.”
Dayo Koleosho was a “useless eater” – a Nazi term – in a distressing scene, where audience members had to feed him by firing peas at him with spoons or squirting pea soup with syringes.
A bird dancing in a gilded cage, unable to escape, was played by DJ Hassan of Corali Dance Company.
Then, representatives of a modern care provider called Paradise Fields proudly proclaimed they were at “the cutting edge of minimal intervention”.
Funny and moving in equal parts, the whole effect was positively overwhelming.
Institutional talk
The event was preceded by a symposium, that asked: “Has institutionalisation ended?”
Valerie Sinason discussed secondary handicap. This concerns obstacles that arise as a consequence of having a disability, such as low self-esteem and poor social relations.
Sheila Hollins and the creative team at Books Beyond Words launched Belonging, a work of fiction about two lonely people living in the community who are brought together by an unexpected event.
Nick Llewellyn, artistic director at Access All Areas, discussed how approaches to people with learning disabilities have moved from control to neglect.
Access All Areas and Books Beyond Words, who organised the day, launched the Belong manifesto, which calls for a better life for people with learning disabilities.
Developers plan to build on the neglected burial site of 1,200 women, men and children who lived, worked and died in an institution.Nigel Inghamreports on the scandal of Calderstones
Calderstones Hospital, in the Ribble Valley, Lancashire, was a large long-stay institution for people with learning disabilities from the end of the First World War.
“We’re treated like second-class citizens,” says Daniel Doherty, a one-time resident of Calderstones.
This pithy statement relates to unfolding moves to build a private crematorium, with a car park and landscaping, on part of the site of the former institution’s graveyard. In this consecrated ground lie the remains of around 1,200 women, men and children who lived and died in Calderstones.
Calderstones – Mersey Care NHS Trust Foundation Trust Whalley site as it is now known – is now home to a low and medium-secure unit, its existence as a large long-stay NHS hospital for people with learning disabilities’ effectively ending in 2000.
At this point, most of its vast main building was demolished to make way for a housing estate and the regional health authority sold the cemetery to a private developer for a knockdown price.
Neglect and vandalism
The cemetery’s 21st century history has been largely a story of woeful neglect and vandalism. There has been wholesale removal of headstones by one of the many private owners over the years, along with a short spell of wanton destruction by local youngsters. Until recently, the site has been allowed to resemble nothing more than a wild, unkempt and overgrown field.
Yet it is the final resting place of well over 1,000 fellow citizens.
There is an added twist, as the graveyard is sited next to a Commonwealth war graves cemetery. Here are the bodies of a number of armed forces personnel who died when Calderstones was a military hospital during the two world wars. The site receives careful attention and is immaculate. This is in stark contrast to the state of the hospital cemetery, through which you have to pass to reach the military graves and memorial.
www.calderstones.nhs.uk
Many walk this route every November to attend the annual remembrance service. It is right and proper to remember the war dead, and to honour them with a well-looked after burial ground.
Recognising and acknowledging the lives of those who died while in an institutional setting is surely of equal worth.
The recent history of these two cemeteries, linked by the same institution, sadly seems to reflect attitudes and values where people with learning disabilities are viewed as second-class citizens.
Dark shadow
Against this backdrop of neglect has entered a new threat. This casts a dark shadow over the future respectful and sensitive use of the cemetery.
In essence, the private owners have been granted planning consent by Ribble Valley Borough Council, to build a crematorium and car park on it.
However, objectors to the development confirmed earlier this year that the whole site is consecrated. Under the 1902 Cremation Act, this would have prohibited planning consent from being granted in the first place. However, this seemed to have been neither investigated nor raised during the sale from the NHS or any planning deliberations. Overall, the principal parties, including the owners, have shown a regrettable lack of due diligence.
The parish council raised concerns over how crematorium-related plans might affect the graves. Ribble Valley, in its report granting consent for a crematorium, said that this was “not particularly a planning issue. This is covered by other legislation with which the developer would need to comply in the event that planning permission is granted and the development is implemented.”
This was presumably on a genuine misunderstanding that the cemetery was not legally a consecrated site.
The issue became urgent after earthworks began last autumn. These were largely halted after consecrated status was confirmed. However, there are strong suspicions that damage has been done. At least one grave – that of former staff member John Newton – was covered.
Furthermore, painstaking research by an objector has established, almost beyond doubt, the location of the garden of remembrance, where 211 former residents are interred. The developers, in their haste and ignorance, mistakenly assumed this was elsewhere and may have already tarmacked part of this.
In April, the owners applied to the Bishop of Blackburn for partial deconsecration; the bishop can grant this under section 22 of the Care of Churches and Ecclesiastical Jurisdiction Measure 1991. This would have allowed building work to continue in an official and lawful manner. Although the proposal respected the known graves of nearly 1,000 former residents, it omitted the garden of remembrance.
Former residents, staff, families, local people, those with learning disabilities more generally, plus friends and supporters contacted the Bishop of Blackburn to express their concerns. Late in May, he rejected the proposal saying: “Submissions received [….] included evidence that there are ashes buried in part of the area relating to the application.”
This is good news for people with learning disabilities and their supporters. In a small way, it perhaps counters Doherty’s concern that former residents are being treated like second class citizens.
However, the story of the cemetery is far from over. It is unclear how the owners will respond and the question remains of how to ensure that those interred are treated in a dignified and respectful way for years to come.
www.facebook.com/letourfriendsrestinpeace
Nigel Ingham works for Pathways Associates CIC on a history learning disability project. Nigel.Ingham@Pathwaysassociates.co.uk
Focusing on ‘basic needs’ is the worst thing a commissioner could do, argues Mark Stables. Bold approaches in the face of budget cuts are the only way to provide sustainable services
Are we “living in troubled times”? I was once asked by someone wanting a meaningful discussion. In terms of social care, anyone would agree that we are.
We would probably also agree that a big part of this is there is not enough money. It is so tough that we get a mention on the news along with health and education.
Peter Gilbert, a great advocate of social work, wrote: “Our task as social workers is to look, see, think and speak positively and beat the predictions of pessimism.”
To be hopeful is not about wishful thinking. It is about being clear about our response to problems and being determined to try always and never give up.
Glen Garrod, the president of Association of Directors of Adult Social Services, has encouraged commissioners to have “more swagger” and he is right if he means we need a confident approach. This requires us to be clear about our role in addressing the situation we are in and upholding the values that underpin what we do.
Big picture
Commissioning is about putting things in place to meet people’s needs. This can mean drawing up contracts, working on the big picture and plans for day opportunities or housing and support. It also covers the work that social workers do with users and carers to achieve certain outcomes.
That sounds straightforward but it is often misunderstood. Now, more than ever, we need to be clear about commissioning and what we should and should not do.
Statements set out everything that people find difficult so they can get support in these areas. A need is not something that I can’t do. A need is what gets in the way of achieving an outcome. As part of the SEND reforms, statements of need have been replaced by education, health and care plans. Statements set out everything that people found difficult in order to get support in those areas. EHCPs from 14 years focus on outcomes in work, health, relationships and independence, making what they want clear and offering support to realise their goals. The Care Act 2014 talks about the role of social care in delivering these outcomes.
What does this mean for commissioning? It means “need” cannot be reduced to something a person cannot do or cannot do without.
When funding falls, it means we cannot think of our role as keeping body and soul together and meeting basic personal care needs. It means we should not reduce day services across the board or ration them.
The role of social care is to support people’s human rights, which means assisting people to have the outcomes they want – those that they have often been denied the opportunity and support to realise. You cannot ration human rights; they do not apply only some of the time.
Being presumptuous?
Commissioners need to design stuff that will deliver outcomes. In Portsmouth, we decommissioned 70% of day services and used the money freed up to support services and activities that provide opportunities in work, health, independence and relationships.
The approach was met with some criticism. It was seen by some as presumptuous: how did we know this is what people wanted? We were absolutely clear that people with a learning disability wanted to focus on these outcomes because they are what we all want. It will mean different things for different people but no one wants to be ill, have purposeless days, have no friends or be dependent.
The transformation has been remarkable. The services now feel as if they belong to the people who use them, and their confidence has grown across the board.
Many more people are in work settings, social enterprises are flourishing and people who were often passive recipients of support are now active contributors to their communities. Projects have been developed by service users. A recent sign of success was that the police approached a local service because they knew this was a group that helped people.
One project, Art Invisible, was set up to support artists with a learning disability. One result of this is that artist Raki Chowdhury has become more communicative, confident and happy. He had previously spent his days in a large day centre, where he wore headphones, had limited engagement and communication, and occasionally became upset.
Art Invisible linked him with Outside, a national organisation supporting outsider artists. This year, Chowdhury took his work to the International Outsider Art exhibition in Paris and, more recently, exhibited in Sotheby’s in Bond Street. His portrait of Jarvis Cocker was sent to the musician who, in a great moment, turned up at Sotheby’s.
Focusing on strengths, designing support to build on these and connecting with the wider world makes the difference.
Plans into practice
Our housing plan has two main themes: changing shape and size; and changing culture and practice. We have done a lot of the first and more than 67% of people are in supported living.
What does this mean in practice? Service users and families have told us that “owning” your home means far more than having a tenancy. It means that, when people come they feel like a visitor, and it does not feel like a staffed service. It means people take responsibility for their homes. We are delighted to be engaging with Gr8 support to make sure people are supported well.
In Portsmouth, we are clear that it is not enough to develop good services and support if the integrated team are not making good referrals.
We have introduced “named workers”, who work with the people they serve to identify what they want to achieve then support them to achieve it. The named workers are proactive – they don’t go away. A named worker may be a nurse, social worker, occupational therapist or speech and language therapist but all work in the same way. Far from creating more work, this has greatly reduced duty activity.
Importantly for commissioning, it enables the market to grow. Very few people ring in a state of crisis saying they are desperate to work in a coffee shop. However, as named workers get to know people and explore their ambitions, they identify goals so providers can take risks and make arrangements to expect referrals. This reduces the need to guarantee funding to a provider to get a service in place. In Portsmouth, we have redesigned support plans and assessments so they all focus on outcome and this is reflected in how services respond.
The relational approach with service users and their families should apply also to providers. That thought will inform how big commissioners want frameworks to be. Like users and carers, providers want engagement. Regular contact and visiting, investing in support and encouraging providers to meet and work together has been of great benefit.
Sometimes, I think we fear over-engagement may compromise our position, but there is no contradiction in being challenging and engaging. Good providers love challenge.
Valuing social workers
In the 1980s, people talked optimistically of social work as a profession. However, more recently, it has become unclear about its core skills and role. At worst, social workers are viewed as people who get in the way. A reductive approach has been taken to assessment.
Service users will benefit from rediscovered clarity and confidence. Social workers need to understand and agree on what make a good assessment and process. They need consistency on what is meant by need, and to unashamedly declare themselves as advocates of the people they support. Only then can they be effective commissioners. When we talk of valuing people, it is good to remember that social workers are people too.
Commissioners and social workers do not divest themselves of responsibility by issuing a direct payment. The information should be pulled together and what is needed should be developed. Otherwise, it would be equivalent to giving each of us a share of the national defence budget to buy our own rifle -….not a good idea.
Services should be put in place only if they have been designed to deliver the outcomes set out in support plans.
In Portsmouth, people often took a direct payment as a way of buying something not very good to avoid having to accept something even worse. We have found that people have no problem with a support plan being drawn up centrally as long as they are involved, own it and there is a range of options that enable outcomes to be achieved.
We are at a critical time when commissioners may be tempted to take the wrong action to meet targets Ð build bigger living units, ration services in a way that ignores individual assessment and think of their role as meeting basic needs to make ends meet. This is a time to assert confidently that we are about supporting people to live fulfilling lives as directed by the Care Act and Valuing People. Focusing on assets of people and their communities and designing everything to support people to use and develop their strengths are the only sustainable ways to deliver savings.
As you might expect, commissioners spend a lot of time arguing for more money. When they do so, they must be clear that, far from undermining efficiency, focusing on independence and being part of community is the only way to deliver sustainable savings.
Mark Stables is service manager for the Integrated Learning Disability Service at Portsmouth City Council
Ray James is the first ever national director for learning disability at NHS England. He talks exclusively to Sean Kelly about his vision with a community focus
Ray James has a crowded in-tray. Among many other issues facing the first national director for learning disability at NHS England are the Transforming Care programme to reduce the number of inpatients in assessment and treatment units, worsening mortality rates and a workforce crisis.
Shortly before this interview, a friend told me she felt sorry for James. She is the mother of a young man with autism and a learning disability.
Why did she feel sorry for him? Because, she said, he is the fall guy for Transforming Care, the national programme with an ambitious target of halving the number of people learning disabilities and/or autism living in inpatient settings such as assessment and treatment units (ATUs).
Transforming Care is entering its third and final year seemingly a long way from achieving this. As the lead officer for the final year, my friend suggested, James’ role will be to carry the can.
He is ready for the charge.
“There has been about a 16% reduction in the number of inpatients over the past three years,” he says. If this much change happened anywhere else in the NHS, “people would be trying to learn from it”, he says – although he agrees that there is “much to be done”.
James is progressing with the 2018-19 plan and promises major decommissioning of inpatient beds in the next year. Some parts of the country have already got the numbers down to the targets in Building the Right Support (the National Plan for Transforming Care) but James says that there is wide variation.
“There is about a five-fold variation in the level of bed provision per head of population. There’s about a 15-fold variation in the rates of admissions.
“So there is definitely more work to do but there are clear signs that things are heading in the right direction. Our challenge is not only about pace but also about reducing the variability.”
James is on secondment for two years (with a possible extension) from his post as director of social services at Enfield Council.
At the time he left the authority late last year, he says “there was an inpatient count of three people [with learning disabilities and/or autism] for a population of 325,000” and two of those three had planned move-out dates.
James gives lots of credit to staff in Enfield for this and is clear why he believes the system can change.
He thinks the frequent focus on inpatient numbers alone is too narrow.
“The programme is often judged in a relatively binary way about inpatient numbers … there are some other important strands as well,” he says. He mentions annual health checks and “the work we are doing around trying to learn from deaths” within the Learning Disabilities Mortality Review (LeDeR) Programme) as well as the STOMP programme, which aims to reduce the unnecessary prescription of psychotropic drugs (CL 31(2): 20-21).
“Fundamentally, I’d like more people with a learning disability to say that they are leading better lives and not in hospitals,” he says. “There might be all sorts of other kinds of metrics that people would look to but, for me, the headline is direct feedback from people about the quality of their lives and their experience.”
What needs to be done to get people out of ATUs and, crucially, reduce the numbers going in?
A priority will be “strengthening the capacity and capability of community-based services, in particular intensive support, crisis support, community forensic services and community learning disability teams”, he says.
This sounds like good news to the many who have been concerned by the reductions in precisely those services.
He also plans to link teams so they can support each other better. Can he transfer funding from inpatient to community services?
“Yes,” he says, adding the caveat that “you need the services to be functioning well in the community to be able to discharge people but also to support and avoid the admissions”.
So far, he says, NHS England has provided £10 million a year (over two years) to be matched by funding from local bodies. “That’s £40 million and I expect there to be a bit more signalled. I also expect us [NHS England] to be clearer about moving some of the money up front now rather than areas waiting,” he says.
He thinks some matters could be addressed in a better way. One is workforce supply and training. He promises “a particular effort around the support and care market to ensure that we’ve got people with the right skills and behaviours”. He wants staff who can provide positive behavioural support (PBS) and who can also, for example, challenge levels of antipsychotic medication prescribed.
Autism overlooked
Another area requiring attention is autism.
“I don’t think we have had a significant or a distinct enough focus on autism and understanding the issues around that” he says. “Of the children and young people in inpatient beds, 60% have a diagnosis of autism and no learning disability, so it is a very significant issue. ” However, he promises no more than “careful thought with people”.
He would like to test some alternative approaches: “What if we didn’t spend any money on a bed – what would we spend the money on? What if we were to invest earlier in parents – what might that look like?”
He considers a future in which parents, carers, support workers and teachers are all trained in PBS and support is much more consistent.
Making plans requires accurate data. However, James notes that there is some conflict between the Assuring Transformation data and mental health data, both of which are produced by NHS England.
“We are working at trying to improve the quality and consistency of that data,” he says, adding that there has been some “helpful constructive challenge” from others, including Chris Hatton, professor of public health and disability at Lancaster University.
The data is not as consistent and certain as he would like but “it is what it is”. Instead of spending energy defending it, he says, “I’d rather be talking to different stakeholders about what we do differently to improve people’s lives”.
Transforming Care is due to end in March 2019. James says he wants people to feel confident that “people with a learning disability or autism or both will remain a priority for the NHS”.
Transforming Care brought in care and treatment reviews (care, education and treatment reviews for children), where the family, agencies and an expert by experience gather to consider plans for a person with challenging behaviour and/or mental health problems.
Asked about their future, he says: “In the last six months, about four out of five care and treatment reviews have not led to an admission.”
Will they continue after March 2019? James says: “I can’t see any way in which they won’t, because of the impact that they are having.”
Eugenics
Given some of the things we have been hearing lately about unnecessary deaths, I wonder whether he thinks eugenics is still alive.
I tell him a story I heard recently of a nurse saying to another, about a man with learning disabilities: “Do you think he would rather be dead?”
James’ face shows distaste. “I find that abhorrent is the first thing to say. My learning from this is actually that it is experts by experience who tend to be the people who change hearts and minds in this space.
“If you are doing training about learning disability awareness, have you got someone with a learning disability involved in the training?”
He says that he knows involving this type of expert works because he has seen it happen.
Preventing unavoidable deaths
The STOMP programme has raised awareness of overmedication. Asked if there should be a similar programme
for constipation, which has led to tragic, unnecessary deaths, James adds respiration, pneumonia, dysphasia
and sepsis, all of which need more awareness.
The solution in his view is to reach mainstream health professionals rather than specialist services for people with a learning disability. Therefore, he plans to connect programmes to existing mainstream services rather than have separate projects.
“I would hope that the work that we are doing around learning from deaths might be one of the places where we get some evidence to help us prioritise,” he says.
James says he has “already influenced the national programme of work around sepsis to ensure that it is more sensitive and thoughtful about sepsis in people with a learning disability”.
Soon after the interview, the LeDeR Mortality Review was published, showing sepsis to be a significant cause of death.
One challenge for James is that he leads a national programme which is delivered in 152 local areas. He says it offers “a blend of high support and, where needed, high challenge”. Local decisions should be made locally, he believes. Nevertheless, he feels that he has the influence and authority he needs.
He describes a health organisation he visited which, after hearing the issues that he raised, decided that “changes in leadership roles” were needed.
Since the publication of the LeDeR Mortality Review, the challenges for James have, if anything, increased. There is a sense of shock within the learning disability world at the worsening life expectancy for people with learning disabilities and there has been some (albeit limited) coverage in the wider media. Learning Disability England has called for a mortality review board to be set up.
However, James remains positive.
“I am really enjoying getting stuck into this,” he says. “There is much to do but I am quite lucky to be asked to do something I care this much about at this point in my career, when I don’t need to be worried about any personal judgments or reflections on me and I can therefore be singularly focused on trying to do the right thing.”
Sean Kelly was chief executive of the Elfrida Society from 2001 to 2012 and is now a freelance writer and photographer.
Following this interview and the publication of LD Mortality Review (published 20th June) Ray James made a response – see https://www.england.nhs.uk/blog/leder/
Far from the often dull safety of mainstream services, Shared Lives offers a radical approach to achieving a normal life. Anna McEwen explains how it allows people to overcome limited expectations and hears about some unexpected achievements
The barriers many disabled people face to having an ordinary life are varied and complex. They run from struggles to simply get up and dressed and needing support to get out of the house to the attitudes of others and finding and holding down a job.
Many factors and circumstances that constrain the ability to live well are deeply embedded in the culture and structures of our institutional forms of public services that seek to offer a risk-free but sterile life.
One way of offering an ordinary life in the community is through Shared Lives. Disabled people choose a carer approved by Shared Lives; the person regularly visits the carer or moves in with them long term as part of their household. While this offers a high degree of support, it can, for some, lead to greater independence.
Stories from family life
Here, two people with learning difficulties and physical impairments talk about living with their Shared Lives carers, what they expected and how life has turned out.
One recurring theme that arises from talking to James Rosborough and Nick Sayers and their carers Andy Cooke, Steve Morris and Tina Hayward is expectations – how they can hold us back, and how they can be addressed to live a healthy and happier life.
James Rosborough: family and friends
Rosborough is 47 years old and has epilepsy and a learning disability. He had lived in specialist residential centres for people with epilepsy all his life until he came to Shared Lives in 2010. He received excellent medical support, and help in managing his epilepsy was crucial to his physical wellbeing. However, there were aspects of his life that he had not been able to explore or develop.
He says: “I was very frustrated at not being able to do my own thing, not go out when I wanted. I didn’t have the independence or the freedom that I wanted.”
Rosborough had no experience of managing the daily tasks and chores of living in a family home, such as cooking, cleaning and going shopping. These were things he actively wanted to do and were part of his wish to live independently. However, he never expected he would have the opportunity for this.
“I never thought I’d be able to have my own house or do the things I wanted to,” he says. “Now I can get the help when I need it that I couldn’t get before. I can do more things for myself now and that makes me happy.”
Rosborough wanted to be more independent and live a life like most people but, having been in residential care for most of his adult life, he sadly lacked the experience of forming and maintaining relationships.
“Before Shared Lives, I didn’t have many friends, but now I do,” he says.
Rosborough met Cooke – a Shared Lives carer – in 2010. Supported by this relationship, he was able to experience and contribute to the many daily routines of life in a community.
His life expanded: his skills and experience grew to the extent that, in 2015, he realised his dream and moved into his own house. He and Cooke chose a house very close to where Cooke and his family live so he can receive support when he needs it and remain fully connected to them. He has a key to the family house and can spend as much time there as he wants; there is a room for him should he need it.
“I like having my own house but can always go to Andy’s house when I want to. I have so much more freedom now,” he says.
From walking to martial arts
Rosborough is more connected to his local community and has become more active.
“I have fewer seizures and my health has improved,” he says. “I’m more active, I get out more and get plenty of exercise. I go to town to the shops, my favourite cafe and the local pub. I like being outdoors. I like bird watching, photography and playing golf.”
His increased physical activity has involved a lot more than walking. In emphatic defiance of the limiting expectations placed on him, Rosborough took up karate and is now working towards his orange belt.
“James was told he’d never be able to do karate and actively discouraged from trying Ð having epilepsy and a learning disability was too big a hurdle to overcome,” says Cooke. “But the instructors wanted to involve him and James is really thriving in his karate class.”
A social company
Rosborough and Cooke have founded a community interest company (CIC) inspired by Rosborough’ experiences.
Since being supported by Cooke to integrate with his community and build relationships, he has grown in confidence and formed his own friendships. Through their company, Local Social, the pair are working to provide that same level of initial support so local people can meet each other and go to social gatherings.
Rosborough explains: “Andy says Local Social is about combating social isolation. I say it’s to help people make friends and get out more.”
Rosborough has, with Cooke’s support, transformed his life and utterly disproven beliefs about what somebody with his impairments could achieve. Perceptions of professionals and wider society about what people with disabilities can and cannot do are easily internalised by the individuals themselves.
Nick Sayers: counting success
Sayers, who has a learning disability, has shared his life with Morris and Hayward for the past nine years. Before this, he had lived in foster care and went to a special needs school.
In Sayers’ words: “It was pretty awful to be honest – I was bullied. I didn’t make any friends and I couldn’t learn properly about the things I was interested in.”
Despite the barriers in his social and educational life, when Sayers changed school and started living with Hayward and Morris on weekends at first, he began to develop skills and interests.
Despite perceptions in some quarters about the academic ability of people with learning disabilities, Sayers has always had an affinity for maths – and a talent for it.
“I like to call myself a mathematician,” said Sayers. Since moving in with Hayward and Morris, he has helped to manage the daily household budget and, for several years now, has used his maths skills in a professional sense.
“I do voluntary work at Barnardo’s, and I am responsible for the banking at the shop I work in. I do a pretty good job I think – I won [a Barnardo’s] volunteer of the year award last year.”
Routine and unpredictable life
As well as growing into his role in the local community and at work, Sayers helps around the house and shares the responsibilities like any other family member would.
“I feed the cat, tidy up and I always make the beds – Tina and Steve hate that job, and they are rubbish at it.”
Sayers’ learning disability, coupled with the extremely regimented experiences of his foster care, meant he was used to daily life unfolding according to a strict plan and expectations.
Hayward says: “Nick likes things just so, and we like to encourage him to express his preferences and choices in terms of things like clothes. He was so used to being told what to do and how to do it, he had very little choice or preference but now he loves to pick his own outfits and buy them.
“The biggest change I’ve seen though, is in how Nick is able to manage challenges to his own expectations. Stuff like there being no milk left or a change in Nick’s bus route home due to road works used to be a cause of massive upset and worry.
“Now, through having lived with us and being gradually exposed to the unpredictable patterns of real life at work and at social gatherings, from a safe and secure base with us, Nick is able to navigate unexpected events.”
Part of an authentic good life is dealing with the unexpected – something Sayers has been able to do since sharing the experience with his Shared Lives carers.
A good life
“A good life comprises our ordinary family, community and work life,” says Alex Fox, chief executive of Shared Lives Plus, the UK network for Shared Lives and HomeShare (https://homeshareuk.org).
“Perceptions abound that some people’s needs, circumstances and backgrounds are just too complex for them to experience these.
“These expectations can underpin the culture of our institutions and are all too often imprinted on and internalised by people with disabilities, leading to a shrinking and suppression of their own expectations and hopes for their lives.
“At Shared Lives, we know giving people access to the routines of an ordinary family home can break the spell of those limiting expectations and give them the extraordinary experiences of living well: at home, in the community, and at work.”
For more information about Shared Lives, visit www.sharedlivesplus.org.uk or email info@sharedlivesplus.org.uk
Anna McEwen is executive director of support and development at Shared Lives
Gaining a family life: how it works
Shared Lives allows a young person or adult who needs extra support to live well, taking part in family and community life.
The person moves in with or regularly visits an approved Shared Lives carer, after they have been matched for compatibility.
Half of the 14,000 people taking part in Shared Lives are living with their carer as part of a supportive household; half visit their carer for day support or overnight breaks.
There are more than 10,000 Shared Lives carers in the UK, recruited, trained and approved by 153 local schemes, which are regulated by each home nation’s care inspectors.
Problems with due process are commonly seen at advice charity CASCAIDr.In the first of a two-part series on be the most troubling issues in health and social care law and practice. Belinda Schwehr gives an overview.
Many issues with basic due process come across the screens at legal advice charity CASCAIDr.These are genuinely concerning, and are likely to be driven by an inadequate number of staff employed to do this work in the statutory sector.
The following problems crop up regularly.
Resource allocation versus actual costs
This concerns the Resource Allocation System, which creates a score that is used to work out how much money can be made available to meet a person’s needs. Problems arise where the figure bears no relationship to the actual cost of care in the local market.
The costing of live-in care is a good example. Allocations may ignore the breaks that a live-in carer has to be given under the working time directive, or the weekly commission that is charged for an introduction to a person who will count as a worker for employment law purposes even though they are regarded as self-employed – and therefore responsible for their own tax and national insurance – with HMRC.
We have one family where a person’s budget has fallen from £60,000 to £20,000 to £3,000 in three years on the premise that her lifestyle had changed.
She was at school for the first year, and the budget paid for care and support during the school holidays. In the second year, she was at home and going to college. She is still living at home and going to college for the third.
One of the items on the scoring sheet is “daily check to see if safe”, so it was clearly not drawn up for people living in their own home.
The reason for this massive reduction cannot be explained, we feel, merely by the fact that she is now able to travel to college on her own, although not home again in the rush hour.
Separate assessments
Another problem is that assessments are carried out by different agencies. This is instead of combined or joined-up ones by staff who have been trained to do more than just one task. Such tasks include carrying out a “carer’s assessment” or “children and families assessment”, or going through the continuing healthcare (CHC) decision support tool process.
This problem is intensified when a person has been placed outside their area through choice or necessity. Local authorities, in the main, are not using their freedom to buy in a statutory assessment from a company acting as the council’s delegate, whose staff might be more than merely competent assessors of single issues.
Experts by lived experience, particularly parent carers, should set up such companies pronto, and take their values directly to the commissioners.
Financial allocation delays
There are longstanding problems with delays in decision-making about financial allocation for the contents of notional care plans, without anything being delivered in the meantime.
This saves councils millions of pounds, and those who need a decision appear to put up with it, instead of requesting “Please get on with implementing what is so far agreed, at least” in the meantime.
Lack of finalised written care plans
The staff left in post after years of redundancies appear to know enough basic legal principles to cover themselves, if the absence of finalised care plans is anything to go by.
The law sees formal council care plans as the record that renders the council accountable in public law terms for the decision as to how much of anything is enough to be seen as meeting a person’s needs.
That has been the law since the late 1990s, and providing care plans is a
duty to all clients under section 25 of the Care Act.
Written care plans are the only possible way to spot: the difference between a defensible care plan and one that is irrational; a care plan that disregards obviously relevant considerations; or one that is unlawful because it breaches guidance or a statutory provision.
What is delivered
Advocates, service users and members of the caring public do not seem to grasp that a Care Act journey is not “done” until a care plan exists, so get lost in the complaints process, instead of putting their collective feet down.
A missing care plan does not just mean that the service user has no idea of how council staff think that the allocation of money or services could feasibly meet assessed eligible needs. It also means that, when it comes to a social services review, neither client nor carer knows what inputs the council or care commissioning group considers it has been paying a provider for.
Furthermore, there is no way of knowing whether that menu has been delivered or watered down, and therefore what has actually been paid for has “worked”.
In legal terms, a provider’s own care plan must be adopted by the commissioners if no other statutory care plan is in place, as part of a council’s section 25 commitment.
Thanks to trends in guidance to commissioners from personalisation gurus, care plans will often be based on “outcomes” only, which is no use to anyone involved in a judicial review.
Direct payments and capacity
Some councils never really thought about capacity when doling out direct payments in the early years of personalisation to any set of parents who were inclined to take on the caring role. The consequence is that entrenched positions have sometimes been adopted.
People who have been holding (in name, at least) a direct payment for years, are now being told that they cannot have one as they do not have capacity. As a result, a parent who is their personal assistant (PA) cannot hold and run the payment and also be paid under the direct payment. This causes massive upheaval.
I believe that this approach is defensible if one starts out with a proper consideration of a person’s capacity to understand what taking a direct payment does – which lets the council off the hook of provision.
But surely this is not the case when a direct payment has been used for years and the adult client has been consensually benefiting from the parent helping to “manage” the payment and the employment relationship as agent for the service user; the parent is not a formal “suitable person” so cannot be the employer and employee at the same time.
Direct payments to relatives
Connected to this are blanket policies that a parent in the same household as the client should not be paid, even where evidence shows that care cannot be purchased in the area for the amount provided by the direct payment.
If the parent were to be willing, no doubt on the minimum wage, to fill that gap in commissioning efficiency, how could it not be regarded as “necessary” to authorise it? We would say it was the best way of avoiding legal action if the council’s commissioners have been so inept as not to manage the market under the section 5 duty, or have been left short of the means to do so by councillors with no knowledge of social care law.
Suspension of direct payments
Direct payments can be suddenly suspended if an underspend is sitting in an account.
Rather than argue about getting it back, the council just says “Get on and spend what you’ve saved up”, overlooking the possibility that there may be a reason for the underspend. This may be because care cannot be secured at any price or that the payment was to made to cover contingencies and fluctuations in the first place.
Most councils’ direct payment agreements build in due process for something as life changing as a suspension of a direct payment. Contracts and employee relations will be irrevocably soured if this process is not respected.
Remedies
Linked to the question of when the decision is actually “made” is the question of what one should do about it if it is thought to be so bad as to be unlawful.
The complaint system is creaking, and the easiest way to avoid getting stuck in it is to ask for something that the complaint system cannot provide. This could be the continuation of services, if these are being provided, or a commitment to provide them pending the conclusion of the complaint process. If this cannot be done, a referral to the monitoring officer is the easy solution.
Our view is that if the decision has been made defensibly – on paper at least – making a complaint is appropriate. However, if the client or advocate can identify an aspect of the situation that is arguably strongly unlawful, it is a sort of Kafkaesque madness to make clients complain first.
Complaints will not conceivably be resolved by a complaints officer without recourse to the council’s adult social care lawyer, who may already have given advice on the matter to the adult services director. Therefore, the monitoring officer should be involved in case independent advice is needed.
Excessive charging
Mayhem in charging has been reported to CASCAIDr, with stories about service users being charged more for a service than it costs the council.
We simply cannot get our heads around how this even happens. Surely the people who make charging software know that the maximum is the cost of a person’s services to the authority, and program in a warning signal if it is exceeded?
We think this is down to block (or group household) contracting having continued, despite the requirement to disaggregate budgets in shared services. We will be focusing on that problem in the coming year as it is what we call a “mindset” issue.
Belinda Schwehr is chief executive of legal advice charity CASCAIDr (www.CASCAIDr.org.uk) and owner of the Care & Health Law consultancy. She has been a barrister, solicitor advocate and university law lecturer
This article is the first of a two-part series. Part two will highlight will look at persistent “mindset” issues in the approaches of local authorities, care commissioning groups and commissioners that affect the delivery of social care and health entitlements
A parliamentary inquiry into assessments for disability benefits had some shocking findings. Charlie Callanan reports and offers some advice to those going through the process
An inquiry by a House of Commons committee earlier this year has found the quality of many of the assessments for disability benefits to be very poor.
It said that this problem had “led to a loss of trust that risks undermining the operation of major disability benefits”.
Almost 3,500 disabled claimants and their carers responded to the inquiry held by the Work & Pensions Committee.
Many individual responses included allegations that the assessment reports written following face-to-face interviews included errors, inaccuracies, omissions and lies.
Examples of poor practice that the inquiry highlighted included a woman with mental health difficulties who was asked why her suicide attempts had failed, and a report about a claimant with mobility problems stating that she walks her dog daily, despite her not owning a dog.
The assessments are done by health professionals working for private contractors. They take place during the claim and/or review process to help to determine entitlement to personal independence payments (PIP), employment and support allowance (ESA) and universal credit for some claimants.
“Untruths”
The committee published its inquiry report, PIP and ESA Assessments, in February. Complaints from disabled claimants included:
Face-to face interviews failed to capture the nature and extent of an individual’s disabilities or their impact on daily functioning
Relevant information shared by a claimant with the assessor not being taken into account
Assessment reports could be inaccurate, and contain errors or “untruths”.
The inquiry feedback includes summaries of many experiences of going through a disability assessment. A quote from one claimant was very telling:
“The report we received was a work of fiction and bore no resemblance to what actually took place.”
Disability charities also fed back some of the experiences of their client groups. The Down’s Syndrome Association was one charity to report very worrying levels of ignorance shown by health professionals who carried out assessments for some claimants with a learning disability:
“Some of the assessors, for both ESA and PIP, need more insight and training with regard to people with learning difficulties …. questions that parents have been asked at the assessments [included]: “How long have they had Down’s syndrome for?” ‘When did they catch Down’s syndrome?’ ‘When were you diagnosed with Down’s syndrome?'”
The government has agreed to a recommendation by the committee to arrange for all face to face assessments to be recorded. It has also agreed to provide more relevant information, such as details about PIP and ESA descriptors (abilities used to calculate limited capability for work), in easy read versions and/or video.
Information and tips
Below are some information and top tips about benefit disability assessments.
The client should attend with a support worker if possible, or a relative or carer – they should be allowed to help the client to answer the questions.
Any current medical evidence and/or supporting information from a social worker or support service should be handed to the assessor. Bring medication and any portable aids.
The health professional will be observing and assessing the client from the moment they meet until the interview ends.
All observations (e g “the claimant kept eye contact” or “the claimant was clean and well dressed”) as well as all replies to questions are used in informing the assessment report.
Assumptions may be extrapolated from an answer to a question. For example, if a client says that she goes to a local shop for groceries, it may be assumed she can engage with other people unaided and deal with money without help – any difficulties the client experiences should be described.
Clients should explain any limitations or difficulties they experience in carrying out an activity. This could include: “I have cut myself while chopping veg and preparing meat, and I burnt myself while using an oven. If I cannot get help with preparing and cooking food, I just heat up a microwave meal.”
Clients should mention any pain or fatigue experienced when carrying out daily activities, and where it takes a long time to complete an activity.
The assessor may physically examine clients, who should not agree to or try to do anything they are not able to do usually.
Clients can contact the health assessment provider after the interview to request a copy of the assessment report.
The Work & Pensions Committee inquiry gave a voice to many benefit claimants with disabilities who found the process difficult and unfair. But the question remains if and when changes will be introduced to make the assessment and reports fairer and more accurate.
All PIP and ESA Assessments Inquiry documents, including the government’s response, can be downloaded from: http://tinyurl.com/y7b936sf
Charlie Callanan is an adviser and writer on welfare rights issues. He has more than 20 years’ experience in the charitable and statutory sectors
 Model behaviour
Model behaviour