A dog’s story helps to explain how to recognise, deal with and prevent difficulties when using the toilet, explain a group of reviewers with learning disabilities
The Trouble with PooMargaret Flynn, Jackie Downer, Karen Horridge and Dave Robinson Illustrated by Beth Webb Beyond Words, 2019, 61pp, paperback: £10; ebook: £4.95
We thought the pictures in the book were very easy to understand and we could understand the story when we talked about what was happening in the pictures. Some of us had slightly different ideas about what the story was saying. Some people thought that touching the dog when she was eating had made the lady unwell; some people thought the dog was unwell because it was eating chips and other food. Having a story of the dog going to the vet first was a nice way of showing that it is good to go and get checked out by a doctor if you are unwell, even if it is a bit embarrassing. The book showed how to know if your poo is not right and how you would feel. There is medicine you can take sometimes but you should also eat healthy food, drink plenty of water and exercise too. You should always wash your hands after touching animals. We thought it was very good that it showed that you can say no to a doctor if you do not want to be examined. We don’t think doctors always explain this. We looked at some of the information at the back of the book. The explanation of words was helpful as well as the chart that showed the different types of poo. We talked about the advice to support workers at the end of the book. We think that support workers should know about these things and be looking out for signs, such as people going to the toilet more or less than usual, and talking to people about it, especially when working with people who might not be able to say if they are in pain or are unwell. We thought the instructions about how to read the book would be better right at the front instead of at the end. It made a lot more sense when we discussed what was happening in the pictures but we had all tried to make sense of it ourselves before we saw that we should be talking about it.
This review was written by a group of people with learning disabilities staying as guests at the
Kingsbridge Road respite service in Kensington, London, which is managed by the Westminster Society for People with Learning Disabilities
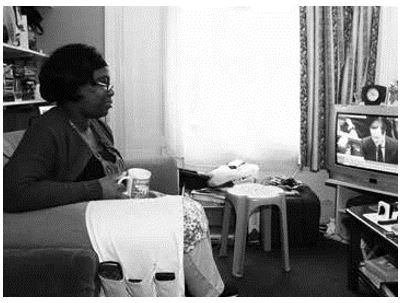
The lack of diversity at TV and film awards ceremonies has hit the headlines. Tracey Harding considers the neglected disability angle of this debate
The British Academy of Film Awards(BAFTA) was criticised recently over its male-dominated best director category, and the lack of actors of colour in any of the major acting categories. While this sparked necessary debate and attention, missing from the discussion was any mention of learning and physical disabilities. A letter to the London Evening Standard, published after the awards evening, eloquently highlighted the omission. Hannah Clarke, a digital assistant at Mencap, addressed the lack of recognition of actors with learning disabilities at the BAFTA awards: “With only 2.7 per cent of speaking characters in popular movies depicted as having a disability, and just 12 per cent of people recalling someone with a learning disability in film, change is not happening quickly enough… “Disabled people like me face stigma and discrimination every day. TV and film can change people’s attitudes towards disability.” In 2019, BAFTA became the first major awards body to introduce inclusion and diversity criteria into the eligibility requirements for their awards. It said productions needed to demonstrate that they had worked to include underrepresented groups in areas including
on-screen presence and in themes and narratives. A positive step was BAFTA’s decision to recognise learning disabilities in this year’s For the Love of Film competition. Now in its second year, this competition involves a nationwide search for people “whose passion for film makes them legendary in their communities”. Winners are invited to spend an evening at the British Academy Film Awards. This year saw an award made to Lizzie Banks, the producer of the Oska Bright Film Festival, a four-day festival in Brighton featuring films made for and by people with learning disabilities, autism and Asperger syndrome. While this is an amazing achievement, as Clarke emphasised in her letter, there is still a long way to go for people with learning disabilities to be recognised in the same way as other groups, and all eyes will be on the awards in 2021 to see if there have been any significant changes in their awareness of disabilities. In a similar vein, and turning attention to another awards ceremony, the Oscars were also highlighting their recognition of diverse creativity, albeit in a small but resonant way. In the last issue, Community Living featured a review of the film The Peanut Butter Falcon, which starred Zak Gottsagen, an actor with Down syndrome (page 27). Gottsagen gave a nuanced performance in a leading mainstream film and, in a historic moment at the 2020 awards, he became the first actor with Down syndrome to present an Oscar. With his costar Shia LaBeouf at the ceremony in February, he presented the Oscar for the live action short film category. Reviewers had suggested that Gottsagen might have received an award nomination for his performance, and his appearance was met with widespread support and acclaim. In the end, as the media focus on recognition for diversity has highlighted, change is essential if we are ever to reach the point where we no longer need to focus on the omission of people with learning disabilities and, instead, can focus on their achievements and talent.
We must collaborate to ensure people’s rights are maintained, including those regarding boundaries around the body and the home. Sally Warren and Jo Giles explain how using a practical guide to the Reach standards for supported living can help you do this
The fundamental principles of supported living are set out in the Reach standards. These voluntary standards were developed by supported living development and training body
Paradigm and are recommended by the Care Quality Commission.
Paradigm has issued a practical guide to these standards, at a time where many are questioning whether supported living works and whether it is at risk of becoming a one-size-fits-all model. In addition, the need to defend the human rights of people with a learning disability and/or autism is increasingly urgent.
The Reach practical guide is designed to encourage all people to stop, reflect and do differently, using the standards. It is described by Dr Sam Smith, the founder of support organisation C-Change Scotland, as “a powerful and much-needed combination of simplicity and raised aspiration”.
For us, there is no better way to support people to reflect and do differently than by meeting them face to face. This always works best when people with a learning disability and/or autism, family members and a range of supporters come together.
To this end, we facilitate Reach standards workshops with people from all over the country, where we encourage them, in the words of John O’Brien, a thinker and writer on learning disability, to: see and believe in people’s capacity to live a good, ordinary life; recognise the integrity gaps and design better ways; and risk trying better ways and reflecting on what happens.
During these events, which are run with a colleague with a learning disability and/ or autism or family member, some common emotions and reactions arise. All our workshops begin with a human rights and freedoms exercise. It is a powerful way to get people to connect hearts and minds.
We ask people to think about their own lives and the everyday rights they enjoy. One by one, these are prioritised by participants, then (with the magic powers of facilitation) we start to remove some of these rights.
As we take away each right, the energy in the room starts to change. “I didn’t realise how much I take for granted,” is the most common comment.
People become passionate; they have a fire in their belly and then – whoosh! – the anger, vulnerability and powerlessness are palpable. People become frustrated. Some withdraw, some even become fiery and some become a little aggressive in their challenge to what is happening.
The rights people typically fight hard to keep include “I can decide who comes into my home”, “I can decide who sees me naked”, “I can refuse medical treatment” and “I can choose who I live with”.
At this point, we ask participants if people with a learning disability and /or autism generally enjoy the same choices and rights. They start to look uncomfortable. “Can people choose who comes into their home?”
“Well… no. Staff must be there and are often not chosen by the person.”
“Can people choose who they live with?”
“Well, no. Sometimes they can but usually someone is referred. They – and the other people living in the house – do not usually have the final say.”
Article 19 of the United Nations Convention of the Rights of Persons with Disabilities states clearly that people with disabilities have the same rights as others, including the right to choose where they live and who with, and to receive support so they can take part in the community.
It is at this point of the workshop that participants describe feeling powerless in a big system.
What can they do? This lack of control is because of money, time, commissioners, support workers, families, social workers and so on. We can see people having an internal debate as they think: “I believe this… but I do that… why?”
The energy in the room drops and we can feel people’s despondent paralysis. People are at risk of losing that fire in their belly right there and then. We understand this reaction. Social care is full of systems that are often too heavy with rules. Cultures can undermine natural ways of supporting someone to live a good, ordinary life. When people feel paralysis and powerlessness, there is a direct impact on the quality of support and possibility.
In our Reach standards workshops, we encourage participants to hold tight to thinking about people’s human rights and work in a way that carries these in our hearts, minds and vision.
We encourage people to keep that fire in their belly aflame and have a whole range of conversations at work – including ones that identify when things are not OK and question why things do not feel right. We encourage conversations and thinking where people try to find solutions or at least little nudges in the right direction.
Don’t pretend things are OK
This involves people agreeing that we should not pretend that all is OK if it is not. Thinking “this is the best we can do” is the slippery slope towards collusion.
Some issues can seem insurmountable in the short term but, when there is space for exploration, questioning and imagination, people always come up with actions. One group of support workers in a Reach standards workshop spoke of a man being referred to a shared home where two people already lived. The two people (who were non-verbal) had communicated very clearly that they did not want him to move in. The support workers had been told the man had to move in because the empty room was costing money. It did not feel right to them. The team felt powerless. In the workshop, they became enthused. They decided to write to their manager detailing the views of the people they supported and their concerns, to be passed onto the commissioner making the referral.
This realisation that they as support workers could do something to advocate for the people they cared about – giving them, in turn, a feeling of self-value, that they had worked with integrity and they could make a difference – kept the fire alive.
We see people’s tiredness, sense of powerlessness and frustration. That is why we also set up the Gr8 Support Movement (https://tinyurl.com/wpkhgks) to connect and value supporters across the country. We also see the effect and the power when people with a learning disability and/ or autism, families, supporters, managers and commissioners come together to identify problems and find solutions together, no matter how small those steps they make might be. We should never underestimate the value of conversations, collaboration and commitment.
Together, we must create cultures in our workspaces where we encourage and grow curiosity, conversations, questioning and the exploration of what is possible because many heads together are often more creative and powerful than one. We need to value those around us who have that fire in the belly – who are brave and stick their heads above the parapet to fight and ask what is right, and do not find excuses to do nothing.
We launched our Reach practical guide and the online toolkit because we are passionate about the power of the conversations of discovery, upholding human rights and people living good, ordinary lives. We are equally passionate about the roles of supporters in doing this.
We have heard some people say that the Reach Standards are “too” aspirational. How can this be if they embrace and keep human rights at the forefront of our minds? If we do not want to lose our own human rights, why is it acceptable for this to happen to people with a learning disability and/or autism? If what is right cannot be fully achieved at a given moment, discuss the obstacles, agree what steps could reduce them and keep them on the radar so they can be addressed fully at the first opportunity. As a recent report says, we need to “understand what the barriers are [to implementing the Reach Standards] and develop strategies to overcome the obstacles, not disregard them” (National Commissioning Board Wales, 2019). n ● A Practical Guide to The Reach Standards: https://tinyurl.com/sm7dref ● To find out more about The REACH Standards training, contact 020 8870 8643 or Gr8SUpport@paradigm-uk.org.
Sally Warren is managing director of Paradigm; Jo Giles is a Paradigm associate
References and further reading
National Commissioning Board Wales (2019) Commissioning Accommodation and Support for a Good Life for People with a Learning Disability Warren S, Cooper O, Schwabenland C (2016) Playing Your Part in Creating Positive Cultures. London: Paradigm O’Brien J (2014) Healing Integrity Gaps. London: Paradigm
People with moderate learning disabilities often miss out, and Liz Tilly has spent more than 30 years addressing this, including setting up charities. She talks to Seán Kelly
Liz Tilly never intended to start a charity. “I never expected that Options for Life would grow as it did,” she says.
Back in the late 1980s, she was galvanised to set up Options for Life by her experiences in a special school. “I was a special school teacher until my mid-20s, and the lack of opportunities for adults when they left school motivated me to apply for Opportunities for Volunteering funding,” she says. The local authority liked what she was doing and, when the initial grant funding ended, renewed and increased it. Options for Life, based in Sandwell, quickly grew, with Tilly as the founder-chief executive. By the time she left in 2008, it employed 60 staff.
People who came to Options for Life could choose from a range of services and social activities to create a bespoke package of support and opportunities to have a full life. There were small day services, support for living at home and support for parents, as well as evening and weekend activities. Tilly says: “I have always had a special concern about people who are on the edge – the people who are not eligible for funding. They don’t get services and they don’t get support.” She means people with a moderate learning disability. “The needs of people with a more severe disability are met through social services-funded provision. The guys who are that bit more able, who aren’t eligible for specialist services, consistently fall through the gaps.”
A unique aspect of Options for Life was its self-build project. Together with Black Country Housing, it developed 10 houses based on Walter Segal’s model of self-build construction, which uses a modular, timber frame system that is straightforward to build and low maintenance. With National Lottery and regeneration funding and support to find a site from the council, the plan took off. Five of the homes were for people with a learning disability and five for neighbours who were entitled to social housing. Also included were a cafe and hairdresser and a new base for Options for Life. The idea was to build a community with support on site.
As Tilly says, “it worked”. The houses were built and everyone, including Options, moved in. All the people with learning disabilities were involved at some level, whether it was in building or painting, using the wheelbarrow or sweeping up. Tilly remembers workmen coming in to the cafe for breakfast sandwiches at 10am and local women having tea and toast while they waited for their hairdresser appointments. Options ran art and parent support sessions both in people’s houses and in their new communal space.
Passing on know-how
By 2008, Tilly had started doing a PhD and decided it was time to move on; she now works part time as a senior lecturer in social care at the University of Wolverhampton, a post she has held since 2013. She was also excited about starting a smaller project, Building Bridges. “I was ready for a change and a new challenge,” she says.
Building Bridges is a co-training social enterprise involving people with a learning disability, again based in Sandwell. Tilly had previously been involved in the Training Partnership Project run by BILD (originally the British Institute of Learning Disabilities) where a trainer and a person with a learning disability deliver training together. She knew people from Options who were keen to be involved. “We got some funding and things took off quite quickly from there,” she says.
“The guys who are that bit more able, who aren’t eligible for specialist services, consistently fall through the gaps”
Building Bridges is still running. It provides training courses for people with a learning disability and staff. It also carries out inclusive research, involving people with a learning disability at all stages, not just in data collection. Tilly says the best courses for those with a learning disability are those that can be applied in daily life so what people learn remains with them. She tells me about a Making Your Money Go Further course, which is about small life hacks on how to make savings. Because the co-trainers have used them, the course has a genuine impact.
Building Bridges also provides training for professional staff. The most popular courses for staff are Supporting Parents with a Learning Disability and Making Easy-Read Materials. Building Bridges has just been awarded an Awards for All grant of nearly £9,000 to continue its research on the barriers to community inclusion for people with a learning disability (see ‘Taking the stress out of going out’, winter, page 11). This funding will enable the group to go out and speak to more people about their experiences. They will write a report on what would help, which will focus on solutions.
The early indications are that barriers to inclusion are rarely to do with the group or event that people are attending. Members report getting a great welcome from churches and other organisations and at activities, but are put off by having to use public transport. Fears of knife crime and other dangers are made worse by witnessing frightening behaviour on buses, and seeing that bus drivers working alone can seem unwilling or unable to curb antisocial behaviour. The group has discussed what makes them feel safer. One is keeping your phone in a different pocket or bag from your money. Then, even if you do get mugged, you will still be able to call someone. The important thing, says Tilly, is that it makes people feel safe enough to go out.
Social life, real life
More recently, she has set up a charity called Jigsaw, which offers outings and other activities, for people with learning disabilities in Sandwell. Its members like the strapline: “For friends, fun and going places.”
It began when some Building Bridges members were arranging a coach trip to see the Winter Lights in Blackpool. Tilly found herself assisting them on an almost voluntary basis. “I said to myself, ‘This should be an organisation’.”
She has organised a regular walking group since the 1980s and also arranges a regular curry club with visits to balti houses. All Jigsaw activities involve volunteers. The only paid staff are the office workers, Tilly and her colleague Jayne Richards. Volunteers are seen not as helpers but as equals or friends. In the walking group, volunteers might help someone lace their boots or assist them on uneven ground if they are a bit wobbly but are otherwise “extra people to chat”.
There is no prohibition on people becoming genuine friends: “It’s not like a service where you don’t give out your mobile number. The idea is that people will keep in touch after the group and maybe even see each other.”
Tilly is well aware of the element of risk but says “we are small enough to manage it”. All volunteers are vetted, have disclosure and barring checks and cannot do anything unsupervised until Jigsaw knows them well.
As Tilly recognises, this is a bit radical: “In most services, you would never let people come to your house or go to their house. You would never do anything on your own with them. This just ‘others’ them. It makes people think they are space aliens.”
Jigsaw prepares volunteers, telling them that if they give their phone numbers out, they may become “flavour of the month” and get a lot of calls at first, and many are fine about that. Tilly adds: “A lot of members are living on their own and going home to empty flats.”
Jigsaw runs weekly activities where people can see friends and take part in social activities. It is making it possible for people to have a real life, says Tilly: “Jigsaw has enabled people to have a bit of a life outside the worry of not feeling you can afford the heating or whatever.”
The charity has received significant lottery funding for development over the next four years. Tilly’s reaction is: “Phew! You can just focus on getting the job done, you know, enabling people to have a life.”
A four-year award gives Tilly a short break from a “great frustration” – forever chasing funding. A problem is that short-term funding is being used to address long-term problems. “But short-term interventions don’t work,” she says. “People need ongoing support and commitment.”
Tilly, too, has shown long-term commitment. She says she would never have guessed as a young teacher that she would still be working with many of the same people more than 30 years later. She has reinvented and developed her work to continue working with people who have known and trusted her for decades. She reflects: “Non-disabled people often move, don’t they? They move areas. A lot of their lives are very transient. Whereas disabled people stay around the same area. And I have stayed around too.”
●● Building Bridges: www.building-bridgestraining.org
●● Jigsaw: www.jigsawevents.org
Seán Kelly was chief executive of the Elfrida Society from 2001 to 2012 and is now a writer and photographer
Fundamental human rights have been protected globally for more than 70 years. So why, asks Simon Jarrett, are the rights of people with learning disabilities proving so problematic?
The purpose of rights is to protect and to empower people – to protect them from harm, such as violence or starvation, and to empower them to live good lives through freedom and opportunity.
There are therefore rights that confer “freedom from” and those that provide “freedom to”. Freedom from rights tend to protect individuals while freedom to rights tend to be enabling, according liberties to people that can carry risks. The fact that these two forms of rights can be contradictory – to achieve personal realisation, a person may sometimes have to shed some of their protective rights to employ their right to take risks – is at the heart of the struggle many people with learning disabilities experience in exercising their rights to live the lives they wish to live. However, as several contributors to this issue eloquently attest, other factors underlie the difficulties experienced by people with learning disabilities concerning their rights.
For Simon Duffy (page 10), human rights are not in themselves enough; they require inclusive communities to enable full and equal citizenship. Sally Warren and Jo Giles (pages 22-23) talk about the dissipation of rights in certain cultures and environments to the point where people struggle to retain them. Clare Palmer and Virginia Bovell (opposite page) attest to the difficulties of applying a universal set of rights (particularly freedom to rights) to people with the most profound disabilities. Political theorist Raymond Geuss (2001) has questioned the effectiveness and usefulness of documents such as the 1948 United Nations’ Universal Declaration of Human Rights and the 1975 Declaration of the Rights of Disabled Persons. Unless such rights are enforceable, with an effective method for enforcement, argues Geuss, they are only an expression of what we regard as desirable, a good idea that we would like to see happen.
“While rights are necessary, they are not sufficient to guarantee inclusion, protection and equality “
Worse, he suggests, such declarations can be positively harmful, creating an illusion of a world in which rights are respected. For the most powerless and isolated, the world is no such thing but, for those of us who are more powerful and connected, the illusion of rights for all is psychologically attractive and comforting.
Who counts as a person?
Where rights apply to “all people”, the question of what constitutes a “person” is paramount. The French Revolution’s 1789 Declaration of the Rights of Man did not include women. America’s Declaration of Independence in 1776 declared the equality of all “men” but this did not include black slaves. In both cases, women and slaves were not seen as fully human.
Today, questions around the full personhood of people with learning disabilities persist. Here in the UK, however much it is claimed that rights apply to all, enduring practices such as incarceration in assessment and treatment centres with little or no legal recourse, denial of the right to family life, education and work, inferior levels of health treatment, and abuse even within community-based services demonstrate that universal rights frameworks can be of little value if people are perceived as lacking full personhood. This is exemplified in the name of the movement campaigning to release people locked up in “specialist” institutions – #HumanToo.
The often unconsciously held belief that people with learning disabilities are not fully human derives in part from our notion of mental capacity. If we argue that a person does not fully belong because they lack the ability to reason, or read or write, or live independently, we are assigning them to a lower level of personhood than the rest of society. Rather than society adapting to whatever characteristics particular humans might have, we construct a society that excludes and withholds rights from people who lack certain “essential” capacities. None of this is to say that rights have no place in the lives of people with learning disabilities. Indeed, they are essential in modern societies where, without them, the risks of discrimination and abuse are extremely high.
However, rights must be enforceable and relate to real lives rather than be illusory ideas about people and the world in which they live. Moreover, it is important to remember that, while rights are necessary, they are not sufficient to guarantee inclusion, protection and equality. To reshape society, there must also be a change in social attitudes that creates a culture of interdependence rather than simple independence. Inclusion is based on but extends far beyond a set of rights.
Its starting point is the individual, their humanness, their right to belong and the adjustments and connections that can be made around them to enable belonging to exist.
Could self-advocates do more to include people with profound and multiple learning disabilities and be more realistic about what they can achieve? ask Clare Palmer and Virginia Bovell
The self-advocacy movement, with its aims of promoting independence and choice, inclusion and better opportunities for people with learning disabilities, is hugely valuable. We applaud its achievements wholeheartedly. However, major challenges must be addressed if it is to include people with profound and multiple learning disabilities (PMLD). For example, the language of campaigns often appears to be directed exclusively at self-advocates who “can talk and work together”, who will “speak up for themselves” and who are “helped to talk about what is happening”.
This seems to rule out people who do not use words – people who struggle to understand or express themselves except through behaviour. Alternatives to words, such as pictures and symbols, can be helpful for some – but not all. They are no substitute for the understanding that comes with knowing someone extremely well. It is usually family members or longterm support workers who understand the nuances of behaviour, gestures and facial expressions of a person with PMLD. Lifelong knowledge of someone and their experiences can be vital to making choices and reaching good decisions.
Yet, as Simon Jarrett said in the winter 2020 issue (We must be honest about including people with profound disability, page 3): “The very people who often dedicate their lives to ensuring their sons and daughters belong in some way have too often been seen as an obstacle to independence rather than a critical cog in the wheel of belonging.”
Greeted with suspicion
There is a long history of family advocacy that has led to progressive developments. Yet we are still often met with suspicion. For example, we recently found ourselves in the uncomfortable position of being criticised publicly for failing people with learning disabilities. We were campaigning for a supported housing development of 11 flats in our borough.
“We were being criticised publicly for failing people with learning disabilities ”
The scheme’s opponents (and potential neighbours) cited the oft-quoted “ordinary houses in ordinary streets” and “a maximum of six people under one roof” to object. They persuaded prominent learning disability advocates from outside the borough to speak against it. Without knowing the facts nor appreciating that a very committed local self-advocacy group also supported the project, they judged family carers’ knowledge and perspective as wrong.
The reality in our London borough is that the most ordinary home is a flat in a converted house or a block – buildings that hold far more than six people. Without this project, 11 people would miss out on their own flat or have to move far away. An ordinary house in an ordinary street is beyond the income of all but a few, and would be inappropriate for wheelchair users and those with additional needs.
Unrealistic ideals
Another area of potential exclusion of people with PMLD and their families is the adoption of “I” statements – for example the Reach standards for supported living. The statements are aspirational and well intentioned, but give little room for context or modification. They are far removed from what can ever be achieved in the lives of many people with PMLD, and may set people up for disappointment or cynicism.
For example, one of the standards states: “I choose how to be healthy and safe.” Our personal experience is very different.
Because of a complex range of gastrointestinal problems, Virginia’s son Danny has to have a severely restricted diet. He will seize every opportunity to eat forbidden foods, without understanding the potentially disastrous consequences. This means he has to be closely supervised and deprived of his liberty around food. He chooses none of this – but it is necessary for him to stay alive. The above statement not only puts words into his mouth (Danny does not use words) but also is simply untrue. It can never be true.
In similar vein, standards 1 and 2 – “I choose who I live with” and “I choose where I live” – belie our own experience. When Clare’s daughter Elinor needed to move out of the family home, there was only one possible vacancy locally, a shared house with three others, also with PMLD, where the intensive 1:1 support she requires was offered. The only choice was to accept or refuse and, because Elinor could not understand the situation, it was her parents who had to decide. The people living there were also reliant on others to make the judgment. This is the challenge: if people with PMLD and their families are to belong within the learning disability community, we need to work in partnership towards a good life for all, whatever the disability.
Virginia Bovell is the mother of Danny; Clare Palmer is the mother of Elinor. Both Danny and Elinor have profound learning disabilities
We are all able to act against injustice, but the way we discuss human rights needs re-examining if we are to truly advocate and build communities, says Simon Duffy
After several decades of progress towards inclusion and human rights for disabled people, we are now in the midst of a difficult period.
The last 10 years in the UK have seen regressive government policies and, unless something changes radically, we can expect this to continue for at least another 10 years. These injustices are not happening on their own – they are combined with general attacks on people in poverty and a failure to address the growing environmental crisis seriously. We are not robots and, for good or ill, we can do self-destructive things, whatever the rational evidence. We are also capable of waking up, changing our minds and getting active. We are all citizens in waiting. So now is a good time to take a fresh look at the language and rhetoric we have used to defend and advance the interests of disabled people – especially those with learning difficulties.
Dark side of pity
We know that the old style of advocacy was the advocacy of pity and this does get a reaction. However, pity is not only patronising but also easily exhausted and, as the well of pity runs dry, humans often turn to darker thoughts. It is only a short step between seeing someone as pitiful and seeing them as dangerous and in need of removal. More recently, disability advocacy has operated in a more egalitarian spirit and has achieved a great deal. Deinstitutionalisation, independent living and disability rights are widely accepted as hallmarks of a civilised society.
Today, in the UK at least, the government has learned how to blunt the impact of these demands and, so far, we have not been able to ignite the interest of the wider public in the multiple injustices experienced by disabled people. I want to propose that this is partly because the language of human rights, while important and truthful, on its own is inadequate. Note the caveats. I am not proposing that we abandon our commitment to rights. I think we will need to supplement it with other ideas – and other ideals.
Limitations
The language of rights has always suffered from limitations. For instance, there seems to be a tension between saying we all have the same rights while also pointing out that some of us are different, face extra barriers, or need more support or money, or that society should be changed in some other way. Increasingly, some are saying that we cannot afford to respect human rights, we do not even have the right to demand them and, if we were really equal, we would not need these special rights. As the saying goes: “You can’t have rights without responsibilities.”
I suspect we are entering a period where we will need to find new ways of defining what is important and what we must protect. We need to recognise that rhetoric is the means of persuading others and we need to find rhetoric that is truthful, ethical and persuasive. Most of all, we need to persuade people who are not within our core group to understand our position. The good news is that we have already done much of the thinking; our failure is not taking our own values and ideals seriously enough nor advancing these ideas outside our special communities.
“Our failure is not taking our values and ideals seriously enough nor taking them outside our communities”
Hunger for community
The idea of community makes sense. We are hungry for community and those with learning difficulties are showing us how to rebuild this, by drawing people together around meaningful actions and paying attention to the gifts and assets in every local area. Restoring the place of the genuinely local neighbourhood community will be essential and we need to reach out to others who feel this need. We need to get behind the ideas of love and family. When all is said and done, it is primarily families who do the work of community life. It is families we go home to; it is a family we aspire to.
Families can get screwed up – like anything else – but the kind of love that families create and inspire can never be replaced. The battles between family advocates and disability advocates are far too damaging to our cause. Understanding what it takes to value families is a ticket to connecting with the hearts and minds of millions. We must claim our citizenship. People with learning difficulties understand the everyday value of equal citizenship better than most. In my experience, they are also among the first to recognise the value of the responsibilities that citizenship brings. We cannot build a better world by waiting for “them” to do “it” for “us”.
Simon Duffy is director of the Centre for Welfare Reform and secretary to the international cooperative the Citizen Network. He recently spoke on this topic when he gave the Norah Fry Centre and Sue Porter Memorial Lecture at Bristol University
Community Living Editor Simon Jarrett previews the latest issue of the magazine.
Our Spring 2020 issue
As I have already said in my most recent blog, (https://www.cl-initiatives.co.uk/editors-blog-march-2020-one-thing-minds/) naturally at present everybody’s mind is on one thing – the Covid-19 pandemic and its huge impact on the lives of us all. I hope that all our readers and supporters are safe and well in these difficult times.
I know that many of you, either through work or your family life, are currently supporting people with learning disabilities through this unprecedented situation.
Some of you live with learning disabilities or autism yourselves, involved in self-advocacy, or peer support or other community action.
I hope we can all support each other through this difficult time as one community, and that Community Living magazine can play a small part in this.
Our next issue, in July, will contain reports from the front line of support services confronted with this pandemic, telling the inside story of how organisations and individuals have coped.
An unsung hero
Meanwhile I hope you will find some things to enjoy, to stimulate your mind, even to provide some moments of escape, in our current Spring issue. Our interview (Supporting the people on edge) is with Liz Tilly, a real unsung hero. Since the late 1980s she has been battling away in the West Midlands establishing a succession of voluntary organisations supporting and involving people with moderate or mild learning disabilities.
Her motivation has been that this group often fall between the cracks, seen as too able to need support and yet struggling to cope in society. This can result in them leading deeply isolated, ignored and poverty-stricken lives, and Liz Tilly has battled for decades (with great success) to give the people she works with the self-confidence, resources and support they need to fit in.
Is everyone included?
At the other end of the learning disability spectrum we continue our debate over whether people with profound and multiple learning disabilities are genuinely included under the learning disability umbrella. Clare Palmer and Virginia Bovell (How inclusive is the learning disability community) talk about their parental experience of feeling marginalised within the learning disability community and how ‘universal’ ideas about learning disability seem not to take their profoundly disabled family members into account.
Try to imagine a life without rights
In this issue a number of our contributors grapple with questions concerning rights.
We air these questions in a spirit of enquiry and open debate, and to encourage a thoughtful understanding and appraisal of rights to ensure that they have an actual impact on the lives of people with learning disabilities.
However, to ask such questions is not to deny the need for rights. We should all take great heed of the article by Sally Warren and Jo Giles (Act together, uphold human rights), where they write about a simple exercise they carry out in their training for support staff. How does it feel, they ask participants, as we remove, one by one, the rights that you say you value most in your everyday lives?
As people imagine not being able to choose who they live with, who comes into their home, whether to refuse medical treatment, they realise how essential such basic rights are to their daily lives. Our shock should not be at how much we take these basic rights for granted, but how a section of the population are so often denied rights the rest of us would not be prepared to live without.
Our editor Simon Jarrett talks about the implications of the Covid-19 pandemic for people with learning disabilities
Obviously, there is only one issue at the front of everyone’s mind at present – the fight against Covid-19 and the extraordinary changes that are taking place in the way we live our lives. The implications of this for people with learning disabilities are as profound as they are for everyone else.
I want to concentrate briefly on three particular issues that arise from this crisis: the emergency Coronavirus bill going through parliament at the time of writing, the work of support organisations in keeping people safe and well during this crisis and the role of hospitals in supporting people with learning disabilities who fall ill with the virus.
Care Act suspension
While everything we accept as normal is no longer normal during this emergency, and all of us must accept restrictions on our rights, entitlements and way of life for the greater good, some aspects of the proposed bill are concerning. Care Act Duties have been suspended for two years. As Learning Disability England have asked, why two years? Better that they should be suspended until two months after the crisis is over.
Of particular concern are the suspension of the duty to assess, provision of direct payments and the blanket removal of duties to meet care and support needs. Whatever changes are made, we need clarity about how local authorities intend to ensure people’s continuing support through this period, and do not see these changes as a green light to simply abdicate their responsibilities, which would be disastrous.
One positive step would be to reduce regulation around contracting to allow providers to take on support for people quickly and flexibly. Incredible support workers
Secondly, I want to pay tribute to all the organisations, support staff and others out there who are doing incredible work in supporting people in the most extreme and unprecedented circumstances. If a person with a learning disability who needs support has to go into self-isolation, they cannot do so alone. Brave and committed support staff are supporting them through it.
The logistical problems are enormous –sourcing food, household items and equipment, staff getting into work, cover for staff who are having to self-isolate at home, trying to manage social distancing – the list goes on and on. I am in awe of the commitment, resourcefulness and courage of people working in the support field.
When this is all over, people must start to recognise who are the really important workers that society depends on to keep everything going for us, and recognise this both in terms of the respect they are afforded and the money they are paid. Hospital treatment
Finally, there is a concern about how hospitals treating people with the Coronavirus will respond to the guidelines on treatment. Clearly if, or when, critical care services are overwhelmed unpalatable and incredibly difficult decisions will have to be made about who gets a bed, or who gets a ventilator, when there are not enough to go around. Italian and Chinese doctors have already had to make these terrible decisions that no one would wish to make – who will live, and who will die?
Government guidance suggests that frailty will be a major factor in these decisions – a younger, normally fit person will gain precedence over a very elderly person who is already in a very frail condition. This seems to me, however unpalatable it is to have to make such judgements, largely just – and I say that as someone whose very frail and elderly mother lives in a nursing home and whose health during this pandemic I really fear for.
However, we must ensure that having a learning disability in itself, and needing support in your daily life, is not seen as a marker of frailty, whatever your age. It is not. Most doctors will understand this, but we have seen enough preventable deaths and ‘do not resuscitate’ notices in hospitals already to know that some doctors don’t. The NHS should make this absolutely explicit in their guidance.
CASCAIDr – the All Adults’ care and health specialist legal advice charity – is going into a different mode for the duration of the Coronavirus crisis.
(Just note during the Covid19 crisis the Ombudsman is closed but once it’s over as out article from Belinda in this current issue says this is a good route after complaints – can be viewed for a temporary period in the current issue)
Small advice charities will become insolvent very quickly, it is feared, without financial assistance.
In all honesty, we can’t hope to cope with NEW individual clients’ legal issues in an effective way. Once the Care Act duties have been suspended and downgraded into powers only (apart from where NOT meeting the needs would amount to a breach of human rights, where it is then still a duty), we will have no legal weaponry with which to fight arbitrariness or blinkeredness, however understandable it may be that these could occur. Rubber bullets instead of ballistic missiles, is how we see the prospect.
We will still offer a legal steer for free, to anyone making a referral on our online referral formhere – for as long as we can – ie concise analysis for sending on to any law firm when seeking advice elsewhere, or flagging up the issue for a council’s own Safeguarding lead and Head of Service.
We will refer people who need ongoing legal work to legal aid law firms with Human Rights credentials and capacity to take work on, in compelling cases. We can’t match what a regulated law firm can achieve, in an emergency, and it’s not ethically rightfor us to charge even our low hourly rate for wasting precious time in trying.
This is going to be our main output for a while: we’re going to provide free template letters online, for the following groups of people to use in their own names – but in the fervent hope of donations, however small, with Gift Aid ticked wherever possible, via https://bit.ly/2WCNHhZ.
The letters will need to be adjusted, to suit one’s individual circumstances, but are intended for the following:
New candidates for a care package, being screened out or left unfeasibly long or told that assessment is not being done unless they would be eligible
Current service users facingapparently arbitrarycuts to existing care plans, or any cuts, implemented without some genuine involvement of the adult and any carer first
Anyone being offered services or a budget that is inconceivablyinadequateorinappropriate in nature
Informal carers being manipulatedorforced into doing more than they feasibly feel able to
Relatives of anyone facing being placed in an obviously unsuitablecarehome
Providers facing unilateral cuts to their fees or refusals to review clients when evidencing increased client needs
If you can think of others that are needed, we will do it! Email ideas to belinda@cascaidr.org.uk please!
We can also provide expert advocacy under s27(2) and s27(3) for anyone who needs it before a revision of a current care plan. We will necessarily have to charge a low hourly rate for that work, but it can be done over the phone or by way of Zoom (online video conferencing software, for which you need only a link and a smart phone or a tablet). Email belinda@cascaidr.org.uk if you need to arrange some of that kind of support.
In the background, we’re continuing to add to our categorised stock of curated LGSCO reportshere – in which our expert writing team explains the legal principles driving the LGSCO’s findings of fault. These matter even if the Care Act duties are suspended – because they are often PUBLIC law and Human Rights based and relevant to the exercise of
Finally, we’re running a page for members of the public to use for reporting GOOD practice and policies as they emerge from Councils and Care Trusts – you can find out about that, here.
Please note that our Trading Company will also be offering top-notch training by webinar/webinar recordings – to councils’ and Care Trusts’ staff. All net income goes to support the charity, of course.
The training content covers how to do what they now must do, as lawfully as possible, with regard to probably the most difficult conversations – and decision-making – that those practitioners and managers have ever had to face … So if you’re a front line worker, a team manager or a senior manager and want that to be available, please mention it to your Head of Service now. The offer will be with all Directorsand Principal Social Workers in the next day or so, and available next week, if we can possibly manage it.
We will do all of this in the hope of donations, however small. DONATE via https://bit.ly/2WCNHhZ
We ask that if you know of any philanthropists interested in social justice, please pass this on to him or her, with a word of approval of our aims and output.
The coronavirus crisis is a challenge to all so photosymbols have opened their new website to visitors and intend to keep adding the latest information in an easy read format . https://www.keepsafe.org.uk/
Books Beyond Words have offered several FREE easy read books on the Corona Virus and associated issues which help the messages get across:
Corona Virus Act 2020 (see below for links to key areas)
A most helpful analysis of the Corona Virus Act 2020 from Belinda Schwehr CASCAIDr . If you want to support her work there is a link at the end of the document or on the website ofcourse
Corona Virus Act 2020 DHSC Guidance to be used alongside any use of the Corona Virus Act removal of duties. It implies serious amount of scrutiny so perhaps now some room to at least question how any such decision is arrived at and to challenge this in relation to the actual needs of the person affected?
CASCAIDr’s translation of the ‘easement’ guidance (link below), issued by DHSC on the Care Act modifications under the Corona Virus Act 2020, includes a useful point that where the LA chooses to revise plans, they must also continue to involve users and carers in any such revision
Mental Health Commission Scotland determines to scrutinise any loosening of the normal duties and ensure any examples are actually exceptional and justified. they have asked that the system includes a formal notification to a scrutiny body each time these ‘easement’ powers are used.
Community Living editor Simon Jarrett previews our 2020 issue – have we been getting it wrong about profound and multiple learning disability, and should we look forward to the New Year with gloom or optimism?
Profound and multiple disability – can we raise the bar?
In our January 2020 issue several of our articles focus on profound and multiple learning disability (PMLD). Melanie Nind and Iva Strnadova (Read more) ask whether we include in a realistic way people with the most complex disabilities in our vision of a society in which everyone belongs. Jo Grace (Read more) reports from the Raising the Bar conference, a national event which aims to develop and apply good practice for this group. And Jan Walmsley (Read more) asks whether, despite the undoubted achievements of the self-advocacy movement, those who are most profoundly disabled have ever had a space within it.
These articles raise important questions which all of us – professionals, campaigners, policy makers, self-advocates and advocates – must look in the mirror and attempt to answer honestly. Dreenagh Lyle’s new book (Read more) about this group of people, who occupy the most complex end of the range of conditions we call learning disability, asks some of these questions. Does the widely accepted social model of disability, which argues that the problems of living with disability are caused by society and its barriers rather than any organic condition, fall short when it comes to PMLD? Does the social model ignore the lifelong, intensive medical and care needs that this group has? When we say that everybody can be independent, work, make their own decisions and choices and be active participants in their communities, are we unconsciously excluding people with the most complex needs from our category of ‘everybody’? To use Lyle’s language have we created a spurious ‘as if’ world, where we try to minimise people’s needs to make them belong as we would wish them to belong, and in the process make it impossible for them to belong?
There is a growing movement to challenge this ‘as if’ thinking and to promote belonging in more sophisticated ways, attuned to the complexities of this group and including in particular their parents and wider families. They have too often been seen as an obstacle to independence rather than a critical cog in the wheel of belonging, people who often dedicate their whole lives to ensuring that their sons and daughters belong in some way. A re-think is needed, and the important work of academics such as Nind and Strnadova in alliance with carers, and the dynamic parent/ professional partnership of the Raising the Bar movement, are a good starting point.
2020 – any room for optimism?
We could all be forgiven for ending 2019 in a state of profound gloom, and looking forward into 2020 with equally profound trepidation. The last year has been characterised by scandal after scandal emerging from assessment and treatment units, hospitals, and ‘specialist’ residential homes. The shocking and utterly tragic cycle of preventable deaths and ruined lives continues unabated. The Transforming Care programme, which was designed to bring all this to an end, proved hopelessly unequal to its task.
As young people have their lives destroyed, some kept in solitary confinement, fed through hatches, straitjacketed and chemically coshed, it is difficult to see a way ahead that is in any way good. The gains of the last two decades can seem to be in full-scale retreat. But, as we have shown repeatedly over the past year, a fightback has begun, led by an alliance of formidable and courageous parents all of whom have had to endure the suffering and ill-treatment, and sometimes even the deaths, of their sons and daughters, under these appalling regimes. Our interview with Leo Andrade, one of these parents, (Read more) shows just why this alliance will, in the end, win. Demonstrations outside the Department of Health, shocking publicity in national newspapers and on television, powerful movements like #humantoo and Rightful Lives are shaming authorities into facing up at last to their responsibility to end this abuse. Community Living will be right behind these campaigns in 2020 – enough is enough.
Mark Capstick was praised by paramedics after putting his first aid training into practice to help a man who had collapsed outside a gym, reports Peter Green
It was business as usual on a wet, windy October morning at The Woodhouse, Integrate’s wood recycling social enterprise in Preston in Lancashire.
A customer who was browsing a selection of timber spotted a photograph of team member Mark Capstick and exclaimed loudly: “Who is this guy? He saved my life a few nights ago!”
Rewind a couple of months. Capstick, a stalwart at the enterprise, attended a certificated first aid course at Integrate along with several of his colleagues. Over the day, he learned about administering emergency medical assistance in a variety of scenarios.
True to his nature, he listened carefully and participated fully in the course then, along with everyone else, went away, proudly accepting his new credential, and went about his life.
Wood recycling is an industrial process that involves access to tools and machinery that can be dangerous if not used properly. It is important that everyone on site knows what to do in an emergency. A knowledge of first aid is just one facet of site safety that we promote and encourage everyone who attends regularly to undertake training in this.
Capstick is a well-respected team member, diligent, conscientious and caring. On a personal level, he is always striving to better himself and this involves trying to eat healthily and regular visits to a local gym.
It was during one of these gym trips that the story unfolds. Capstick had completed his workout and was leaving the gym when he noticed a man outside who seemed to be struggling. The man appeared a little disorientated and was clearly having difficulty maintaining his balance.
Without giving it a second thought, Capstick went to see if he could help and, while he was talking to him, the man collapsed against him. Without hesitation, he started applying the knowledge he had gained on the first aid course, summoning an ambulance and also tending to the casualty.
Capstick had listened to him and realised he had overdone it in the gym, which had caused him to collapse. When the ambulance arrived, he was supporting the man to sit up and encouraging him to take sips of water. Once the paramedics arrived, they praised him for his quick thinking and for remaining with the man until they could take over.
When I was discussing the incident with Capstick, who was his usual modest self, he simply said: “I could see he needed help so that’s what I gave him.”
Annie visits a hospital to find Pete. Doors open by themselves and there are lots of people, wiring and signs, and he tells her something unexpected. By Clare Palmer
The taxi turns into a driveway and stops outside a tall front door.
“Blue door.” Annie knows her colours.
They clamber out and Jane takes Annie’s hand. “We’re going through those doors, up in the lift, and into the ward to see Pete.”
“Ward,” says Annie. “Pete.”
She climbs the steps, but is scared when the door flies open by itself. Inside, there are green walls and a brown floor.
“Come on, Annie, it’s not far.”
Annie feels there is a lump in her chest. It’s getting bigger and heavier. She walks through the doorway.
“Would you like to sit down for a minute, Annie?”
“See Pete,” says Annie. She holds on tightly to Jane’s hand as they walk down the corridor. They stop in front of a shiny grey door.
“Here’s the lift,” Jane says. Just as she raises her hand to press a button the door slides open and two people come out.
There is a big man with a red face, and a woman holding a handkerchief. The man looks at the woman and says something. He sounds cross. Annie wants to tell her about the black marks that run from her eyes down her cheeks.
They get in the lift and Jane presses a button. Annie holds on more tightly as the lift stops and the door opens. She hangs back and they start to close again.
“Oh Annie!” says Jane. “We must get out.”
There’s a man outside, waiting with an empty wheelchair. He puts a large foot between the doors so they bang into it and fly open again.
“Come on, little lady, if you get out we can get in.” He winks at Annie, who likes him, and decides to move after all.
“Annie, it will be your turn. Someday, but not soon. Because you are well now”
“We want Oak Ward,” Jane says. “There it is – it’s straight ahead.” She looks at Annie. “Do you want to hold my hand, or are you OK?” Annie shakes her head, she doesn’t know. She wants to find Pete.
Jane pushes open the door, and they go through. Annie can’t see Pete. There are people in bed, she can see that. Some of them have other people sitting next to them. There are people walking about being busy and people talking to each other. There are machines, and wires, and lots of signs with writing on them. Above her head, she hears Jane saying:
“We are looking for Peter Benson.” The other person must have told her because Jane says: “He’s just over here, Annie.”
And then Annie sees Pete, lying propped up in the bed, very still, with his eyes closed. He looks tired, thin, with deep lines in his face. She runs to him, calls his name. The chair by his bed is too big for her, and Jane helps her into it, but her feet dangle off the floor. Pete opens his eyes, and Annie sees he is happy she is there.
“Hello, Pete!” she says. ”When can we go home?”
His hand moves to cover hers. “We can’t go home, Annie. Not any more.” “Why?”
“Because I’m going away soon,” Pete says. His voice sounds croaky.
“Where?” she says. “Can I come too?” “You will one day,” he says. “But not now.”
“Heaven.” She doesn’t know why she said that. Then she remembers. “Mum.”
“And Dad,” he says. “That’s where they are.”
“Are you going there?” she asks. Pete is quiet. His eyes are shut.
“Are you?” she asks again. He sighs. “Yes, Annie, that’s where I’m going.” “Will you see them?”
He opens his eyes. “Do you think they’ll be pleased to see me?”
“Yes,” says Annie. “When will I come too?”
Jane shifts in her chair. “Annie, don’t you think … ?”
“It’s OK.” Pete says. “Annie, it will be your turn. Someday, but not soon. Because you are well now. Look at me.”
Annie looks. At the tubes hanging down from metal hooks, at the needles stuck into his arm and fastened with tape. And then she points at his face.
“Yellow.”
Pete laughs a little. “You were always good with the colours, Annie. What have you been painting?”
“Pictures for you. Jane’s got them. In her bag.” Jane finds them, and gives them to Annie. “Look, Pete”.
He holds one picture up. Annie points to two pink figures, one small, one bigger. Annie likes pink best.
“Me. And you.” She points to two more, one dark green, the other bright red. “Bad boys. Shouted ‘mong’, and ‘spaz’. You hit them.”
Jane makes a sound, like she’s taking a deep breath.
“It’s years ago, Jane,” Pete says. “We were kids then. I gave them a good thumping and they stayed away. Now she’s got you and the other staff.”
“Look.” Annie shows him the house she has painted. “Home. Can we go back there?”
Pete shakes his head. “You know we can’t, Annie. That’s why I found you the new place.” He rubs his hand over his face.
She puts the pictures on the bedside cabinet. “I like Jane,” she says. “And Bola. And Sue. They look after me.” She holds his hand and sits without saying any more, stroking it now and then. Pete closes his eyes.
A man comes to the side of the bed. He is wearing a white coat and carrying some pieces of paper. He smiles at Annie and Jane.
“Hello, I’m Pete’s doctor. I’ve come to see how he is doing.”
Annie tugs Pete’s hand. “Pete, Pete! Wake up.”
It is hard for him open his eyes, as if they are glued together but, after a few minutes he looks at her.
“Time for you to go, Annie. Need to sleep. You take care now.” His voice sounds strange, fuzzy.
Annie doesn’t say anything. Jane holds out her hand.
“Let’s go, Annie. Say goodbye.”
She pulls herself out of her chair with Jane’s help and blows him a kiss.
“For you, Pete.” Very slowly, he gives her a thumbs-up signal.
Clare Palmer is a family carer in London. She produces film-based training workshops for families and staff who support learning disabled relatives. She writes short stories and is working on a novel
A film with a star-studded cast about a young man with Down syndrome who wants to become a wrestler is clichéd but still a step in the right direction, says Tracey Harding
The annual British Film Institute Festival in October saw the first UK showing of The Peanut Butter Falcon, directed by Tyler Nilson and Mike Schwartz.
The film stars Zack Gottsagen, who met the directors at an acting camp. Gottsagen has Down syndrome, and was so enigmatic and committed that Schwartz and Nilson decided to build their film around him, including incorporating his interests into the script.
A star-studded cast, including Shia LaBeouf and Dakota Johnson, means that the film has received widespread attention. It is currently on release in UK cinemas.
The Peanut Butter Falcon has been compared to a Huckleberry Finn adventure, and its setting in North Carolina against a soundtrack of bluegrass and banjos gives the film an atmosphere reminiscent of Mark Twain’s story.
The film follows Zak, a young man with Down syndrome, who is living in an institution that he is desperately trying to escape from, often with genuinely funny results.
With the assistance of another resident (Bruce Dern), he successfully manages to break out, with the intention of enrolling in the wrestling school of his hero Salt Water Redneck (Thomas Haden Church).
On the road, he meets Tyler (LaBeouf) who is escaping from his troubled past, including thugs who are intent on harming him for a previous misdemeanour. Zak is being pursued by a volunteer at his care home, Eleanor (Dakota Fanning) and, when Zak meets Tyler, the two team up as a seemingly unlikely pair.
Eventually, Zak gets to realise his dream and fights a professional wrestler, but Tyler is brutally beaten by his assailants while this happens. In the closing moments of the film, Eleanor, who has fallen in love with Tyler, drives them all – including Zak – to what is suggested is a new life.
At the Q&A session after the film show, the directors were overwhelmed by the positive response from the audience, and introduced LaBeouf and Gottsagen, who received a standing ovation and gave an eloquent account of his film-making experience.
While the film is optimistic and critically acclaimed, it is debatable as to how far the film challenges attitudes, as sometimes it could be construed as slightly clichéd in its representation of adults with learning disabilities being vulnerable and needing looking after. However, to see a Hollywood film with a central character with learning disabilities actually played by an actor with learning disabilities is a step in the right direction.
On the run: Zak, played by Zack Gottsagen, is desperate to escape from an institution
The Peanut Butter Falcon 2019. Directors and screenplay: Tyler Nilson, Michael Schwartz
A new approach to create inclusive jobs at services for people with learning disabilities – community job crafting – was reflected on at a recent event. Liz Oliver reports
The employment gap for people with learning disabilities is huge. It is estimated that just 5.9% of adults with a learning disability in England are in paid employment (NHS Digital, 2019).
It is well known that the exclusion of people with learning disabilities from paid employment is a problem, but what to do about it is less clear.
In October 2019, people with learning disabilities, researchers and practitioners came together in Leeds to reflect on a new approach to job design called community job crafting.
This is the outcome of a research project called Learning by Doing Together, which was funded by Disability Research on Independent Living and Learning (DRILL). The project was designed and conducted by the University of Leeds’ Centre for Employment Relations, Innovation and Change, human rights organisation Change and service provider KeyRing.
It uses methods of participatory action research and inclusive research to co-design jobs for people with learning disabilities in the delivery of learning disability services. People with learning disabilities took part at every level of the project.
The project team describe the process of making such new jobs as community Job crafting and they hope that other organisations will take it up.
The Leeds event was a great opportunity for the team to preview some of their new toolkits and to hear what people think about the potential of this form of job design.
Fostering inclusive environments
Community job crafting is not about putting people into posts – it addresses the more challenging feat of creating inclusive jobs and fostering inclusive environments.
The idea behind Learning by Doing Together came from the Our Voices, Our Choices, Our Freedom event run by Change in 2014, where 100 people with learning disabilities came together to talk about the abuse of power that happened in Winterbourne View.
A key message from the event was: “People with learning disabilities must be properly employed to work in care settings” (Change, 2014: 23). The idea is that this would address the power imbalances between people with learning disabilities and service provider organisations.
Designing new jobs brings with it an alertness to the wider context of services and service provision, the quality of existing jobs and the power dynamics.
When organisations think about employing people with learning disabilities, they often think about how they might need to change their recruitment and selection practices.
The first step is to design a job that fits well and brings out what people have to offer to an organisation. Participants at the Leeds event were asked some deceptively simple questions such as “what is a job?” and “who is a worker”?
Their reflections on these questions chimed with the thinking underpinning community job crafting – that jobs are not just a collection of tasks but are shaped by ideas about who workers are, how work is done and what is valuable. They reflected on how very few people with learning disabilities have paid jobs so their strengths are not always seen by employers and jobs very often do not fit them well.
Job crafting is a term used in academic literature to talk about the way workers change parts of their jobs. It describes people making changes to their tasks that also alters what work means to them and how it makes them feel about themselves (Wrzesniewski and Dutton, 2001). The team adapted it to describe the way they made a new job with service users. The collaboration made space to think differently about service users and about services.
Job crafting is usually done by one person but the project team added the word “community” because they formed a group of different people who worked together to design the job.
Towards the end of the event, everyone reflected on the afternoon. It had been designed to be open, inclusive and fun. The team were pleased when one participant noted that the activities gave people confidence and connected everyone.
Those taking part seemed to enjoy it, talking about thinking differently and questioning their preconceived ideas. People were keen to know more about community job crafting, particularly about how it works in practice. They were also keen to network and connect with each other. The team will be running more events to share other parts of their toolkits.
Dr Liz Oliver is a lecturer at the Centre for Employment Relations, Innovation and Change (CERIC) at Leeds University Business School
References
NHS Digital (2019) Measures from the Adult Social Care Outcomes Framework, England, 2018-19. https://tinyurl.com/yeoycugk Change (2014) Our Voices, Our Choices, Our Freedom. https://tinyurl.com/yerlw8wf Wrzesniewski A, Dutton JE (2001) Crafting a
job: Revisioning employees as active crafters of their work. Academy of Management Review. 26(2):180
Little research on how to improve clinical care from the perspectives of people with learning disabilities or autism has been carried out. A project led by Alison Doherty and self-advocacy group Pathways Associates sought to address this
Numerous studies have shown that people with learning disabilities and/or autism have higher rates of long-term health conditions and die earlier than other people in the general population (Emerson and Hatton, 2013).
Despite this, it has been shown their access to health services is poor and their health needs are often unmet.
In addition, little research on this from the perspectives of people with learning disabilities or autism has been carried out. To address this, a co-produced research project to look at facilitators and barriers to better healthcare was undertaken in the northwest of England.
People with learning disabilities were involved in the co-production of research design, questionnaires and easy-read research findings.
Findings
Hospitals
Participants found hospitals overwhelming and impersonal, and they caused anxiety in several people.
“Sometimes you have to make sure the room is a bit quiet, so you are not getting a bit anxious.”
Participants said they had been anxious about finding their way around hospitals, which could be an “absolute nightmare”.
Families indicated that they often needed to visit several hospitals to see different healthcare teams and this was not helpful.
“All the different hospitals. Each time, there’s different people. That impacts. So, for my daughter, my wife and myself are supporting her. She would really struggle and her health would be impeded.”
Time
Another barrier was waiting times.
“You can’t get an appointment. Then you have to wait about two weeks.”
How much time patients could spend with clinical staff was also raised. Some felt they spent more time with their GP than hospital staff; others felt they did not get enough time with either.
Communication
It was sometimes difficult to describe symptoms and people needed more time to process information, particularly if they had other disabilities such as sensory and physical impairments.
People were positive about staff who knew them well, which helped put them at ease.
“He also knows how to treat you if you are uncomfortable with certain things.”
Some staff – clinical and non-clinical – did not understand needs and some people had been treated poorly as a result.
“The way they said it. In a nasty way. ‘You have to come in at 8 in the morning to make an appointment.’ ”
Doctors would often talk to a carer or support worker rather than the patient, and this was more likely to occur in hospitals. A good doctor was one who “will look at you and talk to you, not talk to the support worker, because you need to know what’s going on”.
The lack of up-to-date information in easy-read formats was a particular concern.
“If our son or daughter did not have us as parents going through all this material, they wouldn’t be attending anything. Because they wouldn’t know.”
Not everyone had heard of or had health action plans, health passports or health checks. Participants spoke of the need for consistency in how these were accessed through their GPs.
Fear
Fear was a common barrier and this included fears of needles, health checks, cancer screening and hospitals in general.
People were also embarrassed to talk about their symptoms to staff.
“It’s embarrassing talking about it … Talking about bowels and stuff.”
The consultation rooms provided by some pharmacists were viewed positively.
“My chemist has got a private room where you can go in and talk to the person.”
Technology
Automated phone systems can be a barrier to making appointments, particularly when a caller has to choose between multiple options. Touch-screen technology caused confusion.
There was resistance to and mistrust of automated and online services.
“Not everyone has access to computers.”
“No – we don’t trust anything.”
Face-to-face interactions and “personal contact” were preferred, although some welcomed online healthcare tools and apps.
Social support
Social support is an important facilitator and those lacking a support network and/ or living alone may not act on health concerns, as a carer suggested.
“People who are in supported living … at times don’t receive appropriate health care because staff don’t support them to attend those appointments.”
People with learning disabilities and/or autism often rely on others to support them to attend appointments, so some allowance should be made for a lack of attendance.
Participants identified the need for co-ordinators to work with people with learning disabilities and/or autism.
“It comes back to that healthcare co-ordinator. Somebody who will act as your support. And maybe unofficially your advocate almost.”
Some people had not considered using pharmacists for help and support.
Training
People with learning disabilities and/or autism need to know how to check for cancer symptoms and how to use medical equipment so could benefit from training.
It was thought both clinical and non- clinical staff needed training. It is critical that any course is provided jointly with people with learning disabilities and/or autism.
Funding could be a barrier.
“We asked our local health nurse and she said: ‘Bad luck, guys. There is no money in the budget to train you up to train us up.’ ”
Additional needs
The participants also spoke of barriers to accessing healthcare that were related to conditions, such as a lack of home visits for people with agoraphobia.
In addition, some said dental forms needed reviewing as they had been charged wrongly for dental services.
Conclusion
There are several barriers and facilitators to improving healthcare experiences for people with learning disabilities and/or autism.
These often relate to how staff relate to and treat these patients. Raising staff awareness and improving their understanding of patients’ needs, for example by providing them with information in easy-read formats or allowing more time in consultations, would greatly improve the experience.
Emerson E, Hatton C (2013) Health Inequalities and People with Intellectual Disabilities.
Cambridge: Cambridge University Press
The research was part funded by the National Institute for Health Research (NIHR), Applied Research Collaboration North West Coast (ARC NWC), NHS England and the Lancashire Research Institute for Global Health and Wellbeing (LIFE) at the University of Central Lancashire. Alison Doherty receives funding from NIHR and ARC NWC. The views expressed are those of the authors
Alison Doherty is research associate – evidence synthesis at the University of Central Lancashire
People with learning disabilities can rarely access private rented accommodation, yet it can be right for those who can live independently and faster to secure than other homes. Care Housing Association can make all the arrangements, says Matthew Eddisford
The provision of housing for people with support needs has long been limited to certain traditional models, most of which require significant initial expense and longer-term commitments from landlords and partner agencies such as local authorities and care providers.
Unfortunately, this means it can be difficult to secure, particularly for people who require something they may not be able to access easily through existing routes or those who need housing in a matter of weeks rather than months.
Care Housing Association has added Faster Housing Solutions (FHS) to its menu of housing options for people requiring support but who are more independent. FHS searches for housing in the private rental market for people who perhaps do not need significant adaptations to their home and are looking to move relatively quickly.
Care works with private landlords and agents to find good-quality properties where people want them. Landlords have the reassurance they are supported by a reputable housing association.
How to apply
How does it work? The starting point is for a person to let Care know exactly what they need and want from their future home.
Care then determines if the application is suitable for FHS. If not – for example if someone needs significant adaptations – we will let the applicant know and perhaps advise them about our alternative models of housing or point them in the direction of other, more suitable options.
If FHS is suitable, great! We work with the applicant to find a home that meets their needs and aspirations. If we find a property that everybody agrees is suitable, we can work quickly to secure it.
Care’s involvement does not end there. Once the property has been secured and the tenancy agreement signed, the person will benefit from a housing management service designed to ensure they can maintain their tenancy.
The service includes:
24-hour repairs and maintenance service
Ongoing tenancy support and advice
Access to other tenant benefits such as the Care Foundation, which provides £500 grants to tenants for items, services and experiences that improve their lives
Peace of mind offered by a reputable, charitable landlord.
The only disadvantage for tenants is that we can offer only assured shorthold tenancies via FHS. As we do not own the property or hold it on a long lease, we cannot offer more security of tenure.
However, we will work with landlords and their agents to ensure tenants can stay in their home for as long as possible and for as long as they wish.
Who is eligible?
We want FHS to be open to as many people as possible. However, applicants for the scheme must:
Receive at least 20 hours of support per week. Where the support level drops below this threshold, we may still be able to help, so please contact us
Not require any adaptations to the property. For this reason, FHS is not suitable for those who require specialist equipment in their homes, such as hoists and tracking
Want to live in the north west of England. We are not offering FHS outside Lancashire and the surrounding areas. FHS is a new concept to Care, but one we believe can be a great success and crucial to people not being catered for by supported housing providers. We found our first “FHS tenant” a property in Preston in September and are working on new applications as we speak.
http://careha.org.uk/
Matthew Eddisford is chief executive of Care Housing Association
Contact Care Housing Association
Faster Housing Solutions
Contact project manager Doreen Singleton on doreen@careha.org.uk General enquiries
Filmmaker Beth Richards was inspired to make a funny yet powerful film about why it is difficult for people with learning disabilities to get on television, which she hopes will make those in the industry give them a fair chance
There aren’t enough people with learning disabilities on television.
My animation, The Audition, shows the barriers they meet right from the start of the process when they try to go to auditions.
There are simple things people in the arts can do to be more inclusive once they give it some thought.
I was a research associate at the University of Bristol. When they asked what I wanted to find out about, I said I was interested in why I don’t see more people with learning disabilities on television.
After I had done my research, I wanted to share my findings in a fun, visual way that would make people think.
I was able to make it because I had such good support to help me with my ideas. I worked with a research partner at the university during the whole project.
Getting through the door
I hope people who see The Audition will be amused but afterwards remember the image of my character’s body unravelling.
This is how it feels when people speak to you in jargon or technical language, when you realise no one has thought about accessibility and are not really giving you a fair chance.
Hopefully, they’ll also use the tips at the end of the film.
A lot of people who have seen the film say the unravelling body is powerful, as it shows how disabled people can feel when they are excluded. People with learning disabilities might find the film helps them explain how they feel if adjustments they need to be included aren’t made.
Messages through film
I’ve been in Bristol’s Misfits Theatre Company for years and we have been filmed quite a bit.
We have explained the findings of the 2013 Confidential Inquiry into Premature Deaths of People with Learning Disabilities, carried out at the Norah Fry Research Centre at the University of Bristol. This discusses how “health is everybody’s responsibility” for NHS England – health professionals must recognise they must provide the same level of care to people with learning disabilities as to others, and not make rapid assumptions about quality of life or the appropriateness of medical or social care interventions.
The Misfits company also looked at the importance of good working relationships between people with learning disabilities and their personal assistants or support workers in our short film A Good Match (https://tinyurl.com/y68rnqx7).
I also made a short film, I Hate You, Jargon!, which shows a meeting get out of control, which has been described as “Beth Richard’s passionate rant against use of jargon”. In it, I say: “Get rid of the jargon that you speak. On and on and on it goes … For God’s sake, speak in easy English, and make sense!” (https://vimeo. com/246467274).
We’re always thinking of ways to get messages across clearly. I found I was comfortable in front of the camera and like the way film can be accessible to everyone.
I interviewed people at the Oska Bright Film Festival for part of my research. We asked David Parker from Carousel, the company that organises the event, for feedback on the leaflets we made about the film project. He was very supportive.
As part of that conversation, he invited me to take part in a panel discussion and show my film at the 2019 festival, which is how I came to screen The Audition and talk about it at the co-production session this year.
People from around the world were there – it was a great way to tell them about the research and about what needs to change.
This article is adapted from Too Few People with Learning Disabilities are on Television – So Let’s Make Auditions Accessible, published by Learning Disability Today at https://tinyurl.com/w7oeeqy
Richards B, Steel M, Mason-Angelow V (2018) Actors with Learning Disabilities Say: “Give us More Roles on TV”. Policy Report 31. University of Bristol.
View The Audition and read the full report and an easy-read version at: https://tinyurl.com/ t7dac96
The Oska Bright Film Festival – now accredited by BAFTA – was bigger than ever this year. Lisa Wolfe saw how identity was central to learning disability film this year around the world
There is a perplexing, baffling, endless interior to everyone in their mind/mental state, which is almost incomparable to your physical health and what you present on your exterior which can be a superficial and fake representation of yourself.”
The themes of Eleana Re’s keynote speech at the 9th edition of Carousel’s Oska Bright Film Festival resonated throughout the four days of this extraordinary event. Re is a visual artist and film-maker who has atypical autism.
Her questioning of identity, how we present ourselves in our daily lives and how we are perceived, was common to many of the films shown over the four-day event in Brighton. It’s an issue everyone can relate to – the pressure to fit in is huge.
The festival opened with It Me, which explores how learning-disabled people navigate the world today. It included Tamsin Parker’s funny and heartfelt Force of Habit, in which she identifies with the Mexican bandit from The Good, the Bad and the Ugly, an outsider who struggles to understand his motives as she does hers. Mixing animation with narration, it is an effective call for greater awareness and kicking down barriers.
Shakespeare in Tokyo by Australia’s Bus Stop films is a beautifully shot story of a Shakespeare fan with Down syndrome exploring the culture of Japan and the effect he has on the lives of strangers he meets. His confidence and contentment are at odds with his brother’s urge to shield him from public encounters. The positive messaging was popular with the audience and the central performance captivating enough to overpower the unnecessarily sentimental piano music in certain scenes.
In 2017, Matthew Hellett, head programmer of the festival, introduced the Queer Freedom strand to explore the intersection of queerness and disability.
Six films were shown in this category including Born to Dance With an Extra Chromosome, a documentary about Drag Syndrome, a performance group that is transforming the drag scene world wide. Each artist has a fully defined drag character and totally owns their performance.
It was thrilling to watch how they connected with audiences. In the aftershow panel discussion, we heard the shocking story of how they were banned in some American cities for not confirming to accepted ways of being for learning disabled people. If the revolution is coming, Drag Syndrome might well be leading it.
Meeting across the world
New to the festival this year was a networking breakfast for film-makers from abroad. Oska Bright’s international reach is huge, with films screened from 17 countries in total, including Croatia, Iran, Japan and Russia.
The breakfast brought visitors together, including Germany’s Barner 16 with whom Carousel and Oska Bright have a long relationship. Kai Boysen of Barner made a plea that “whatever happens between the UK and Europe, we need to keep on building a global community for learning disabled artists”.
The dance and music screenings, which showcased a broad range of talent, included Daniel Wakeford’s music video It’s a Wonderful City, filmed in Brighton and sung with infectious passion by the popular TV star.
Kill Off, by Genevieve Clay-Smith, features a bravura performance by Jamie Brewer as young dancer Sonja, who is crazy about krump, a street dance style. As with Shakespeare in Tokyo, an overprotective older sibling learns to let go of fear. Street smart and self-aware, Sonja is a role model for us all.
Your Rocky Spine is the latest in a series of haunting dance films by Shropshire’s Arty Party. Three couples dance across the landscape in finely choreographed duets, with close-ups of hands and bodies that echo the rocky terrain. It culminates in a courtly waltz scene in a country hotel, Downton Abbey style, with not a step out of place. As Arty Party said in the post-show panel discussion: “We did it so many times to get it right. That’s why you enjoyed it.”
Perhaps the most intimate and revealing screening was Portrait of the Artist. Here, fiction gave way to personal experience as visual artists explained their practice in nine illuminating short films.
Most powerful to me was Mary by Erica Sutherland, in which Mary Decesar told of her early years in the US school system, being put to work in a military base and how art has sustained her through hard times.
Her drawing and embroidery are expressions of things she loves and of her world view. “I started to get proud of myself by making things,” she said. “I always liked that, being an artist.”
Studio creativity
Two films focused on studios where learning disabled artists are encouraged to be creative in whatever medium appeals to them.
Tanya Rabbe Webber, a prolific painter herself, runs ArtStudio01 in Shrewsbury and mentors newcomers and experienced artists. In Spain, La Casa de Carlota employs learning disabled artists to work on high-profile commissions for international brands. The film Design Ability takes us through the process from pitch to finished campaign.
The art, such as that by Rose Wylie or Hanna Hoch, is astonishing but it is how the design company applies it that makes the campaign a success. As with many of the more accomplished films in the festival, high production values and skilled editing make a big contribution to its impact.
An example of this is the excellent Oddlands, by Australia’s Bruce Gladwin, winner of the Audience Choice Award. Every frame is masterful, the sound balance is perfect and the interior scenes beautifully lit. This story of a future toxic world is compelling, scary and acted with aplomb. It deserves to be properly distributed as an example of great film-making that just happens to have a cast of mainly learning disabled actors.
It is fantastic that films of this calibre are being made. Production firms, talent pools and audiences are realising the value of difference. At last!
For me though, the films made in bedrooms on low budgets have an aesthetic that is honest and, occasionally, more radical. The work of Danny Smith, winner of this year’s Dance Film Award for Time to Leave and animator Teagan Nash’s The Snowball Effect are good examples.
Triumphant
As the Oska Bright Film Festival shows, there is space for everyone and everyone’s invited. From sessions for children and schools to a late-night screening of experimental film, surgeries with industry experts, a European screening and a triumphant awards party, Oska Bright’s 99 films showed how rich and eclectic the learning disability film scene is worldwide.
Think “talent added” and, as Re says: “You’re enriching people’s lives with your art as well as your own life. Just believe in yourself and go for it.”
The next Oska Bright Film Festival is in 2021. To submit a film, go to www. oskabright.org, where you can find out about 2019’s winners. A round-up video of this year’s event is at http://tinyurl.com/ yynsgvb7
The Oska Bright Film Festival is produced by Carousel, a learning disability-led arts company based in Brighton. It is funded by the BFI and Arts Council England
Looking at the histories of two institutions that closed recently gave cause to reflect on life today and the past’s influence, say Claire Jackson and the Hidden Lives Remembered volunteers
The two places whose history we researched were Middlefield Hospital, open from 1866 to 1992, and Hampton Manor, a residential home, which was open from 1952 to 2007.
For this article, we are going to focus on Middlefield Hospital. You can learn more about Hampton Manor at our website www.hiddenlivesremembered.com.
An institution, in this case, is a place where lots of people live together in the same building(s). They had usually been sent there for one of three reasons, and there was always a focus on making the people “better” in some way:
To be cared for, like at a hospital – the goal was to make the person “better” from a condition
To be trained and educated, like at a boarding school or university – the goal was to make the person a “better” member of society through gaining new skills
To be kept away from the general public, like at a prison – the goal was to train the person to behave “better”. The aim was also to make society “better” by locking away a person who was seen as dangerous in some way.
Learning disability institutions aimed to do all of these three things. Many of them started out as private asylums, then they became institutes and last they were hospitals and part of the NHS. You can see this in how Middlefield Hospital changed its name over the years:
Dorridge Grove (1866-1872), a small private asylum
Midland Counties Idiot Asylum (1872-1901)
Midland Counties Asylum (1901-1911)
Midland Counties Institution (1911–1948)
Middlefield Hall (1948-1959), taken over by the NHS
Middlefield Hospital (1959-1992). People were sent to places like
Middlefield Hospital to make them “better” members of society, with the aim of them being eventually discharged back into the community.
Long-term institutions
Although some people did return to the community, many ended up living in these institutions for a very long time, if not most of their lives.
Some institutions housed more than 2,000 people. Middlefield was a lot smaller, with a maximum of 275 people – but that’s still a lot more than most people would wish to live with.
They were treated as patients and lived on wards but were disabled, not ill. The idea of a hospital is to make someone better from a condition, then they leave and go home. But you cannot cure learning disability – and nor should you have to. This meant that treating people with this medical model was never going to work, as the people would never be cured – and would potentially never leave.
A report in the 1960s on Middlefield Hospital said the length of time people had been living there ranged from a few weeks to 73 years.
For most of us, we live, go to school, go to work and socialise in different places with different people. There can be some overlap but we usually have a few different spaces and places where we feel we belong. We can call these “spheres of belonging”.
However, the residents lived, slept, went to school, went to work and socialised all in the same place, with the same people. They sometimes went out on holidays or trips, but their lives were mostly lived out within the institution’s walls, in a single sphere of belonging.
The wards were often low on staff, so the residents usually followed a set daily routine and received little personalised care or individual attention. They did not have a lot of personal opportunities and did not get much choice in what they wanted to do, where they wanted to go or even what they wanted to eat. They did the same as everyone else or they went without.
Moving out: pleasures and pitfalls
When the institutions started to close in the 1980s and the residents moved out into the community, some of them found it quite difficult.
Middlefield had built a training unit called Freshfields to help the residents learn the skills they would need, such as using money, cooking and cleaning, but most of us get to gain these skills over a lifetime, not just in a few months.
For some, suddenly having their own room after years of sleeping in a ward or even the idea of choice took some getting used to. They had many more opportunities but had not really been shown how to make the most of these.
The residents were also suddenly dispersed, and some went back to where they had originally come from, although they hadn’t lived there for many years, and old friendships forged in hospital were lost.
On the whole, however, moving into the community was a good thing. The former residents were able to start enjoying many of the freedoms and choices that most of us just take for granted. But, by this point, many of them were quite old, and nothing would ever be able to make up for the potential opportunities they had missed out on because they had lived their lives in an institution.
Albert Goodall had lived at Middlefield for nearly 70 years when he left in the early 1990s. He had moved there when he was only 10 years old.
He told a paper in 1992: “For the first time in my life, I can do things I want to do, and I like living with a lot less people.”
He was a very popular member of the community and lots of people came to his funeral when he passed away a couple of years later.
Hidden Lives Remembered
A fantastic group of volunteers have worked on this project, many of whom have a learning disability. They have had the chance to gain skills in archive research and doing oral history interviews, where we record history through asking people about their lives.
They have also been involved in public speaking, and a group of us went to the Open University’s Social History of Learning Disability Conference in July to talk about the project.
Hidden Lives Remembered and me: how the project affected our volunteers
Kathleen O’Bryan: Seeing pictures from Middlefield really got to me. The beds in the wards were really close together. There wasn’t much dignity. I didn’t get to study history because I went to a special school where it wasn’t taught. I had never been to an archive or done anything to do with heritage before, and I’ve loved this opportunity. I really enjoy interviewing people, and it has helped me build my confidence. My daughter has said she is really proud of me.
Keith Webb: I went to a dance at Middlefield in the 1980s. What I saw of it, I didn’t like. It was a bit dowdy. I’m glad it’s gone. When I was sick as a child, I had to stay in a hospital. If I was naughty or went for a wander, I was locked away. I still hate going to hospitals today because of that. I feel sad for these people who had to live in a hospital.
Mariza Webb: Before this project, I didn’t know that Middlefield existed. I wanted to learn about how people with learning disabilities used to live. I was shocked by how some people died young in institutions in the early days. I enjoyed being shown around the archives and seeing the different types of things that they have there.
Gilbert Moult: I knew of Middlefield before the project, but I didn’t know much about it. I was interested to learn more. I was shocked by how it used to be called an “idiot” institution. It’s probably a good thing that these places aren’t there any more, but some of the things that went on, like abuse by staff, are still happening today.
Colom Benham: I liked looking at the old photos and newspaper articles. One that stood out to me was about Christmas dinner at Middlefield in the 1970s. The catering manager was annoyed at the staff doing things their own way and binned their turkey! It showed that she had a lot of power and the staff didn’t always get along. I’ve enjoyed doing interviews and listening to people’s stories.
Jennifer Brown: Even though I have worked with and known people who lived in these institutions, I didn’t know much about them before the project. I was surprised by how little I knew about them, and that a lot of other people don’t know about them either. I strongly believe that the people who lived at Middlefield and Hampton Manor should never be forgotten, and we need to make their stories heard.
Hidden Lives Remembered is run by Solihull Action through Advocacy and is supported by the National Lottery Heritage Fund
A group of individuals who do not receive community support researched what stops people going out and getting involved in their local area. Liz Tilly and the Building Bridges Research Group found what made them anxious and looked at how to address this
Feeling alone and not connected to others where you live affects many people, especially those with a learning disability, and has become an important political issue.
The Building Bridges Research Group – eight people who do not receive home or community support services – carried out research to find out some of the things that stop us getting involved in local places with local people where we can make and keep friends. We made picture cards and used photos to show the findings of our group discussions.
There were positive experiences of joining in and using community places where we were made to feel welcome, such as church coffee morning drop-ins, clubs specifically for people with a learning disability, libraries and sports centres. We liked it when people said hello, talked to us and treated us with kindness.
The sports centre gym was very important, as were activities such as swimming and keep fit classes. Gym membership cards, issued to people who receive disability benefits that allow free off-peak use of the gym, were valued for giving us status as belonging to a local community facility. Pub use was limited for a number of reasons, including not feeling welcome.
Feeling Safe When Out
We said that needing to feel safe when out was really important. Many of us expressed fears about being out in the dark, which was made worse by hearing about news reports of stabbings, acid attacks and shootings. People were also afraid to use alleyways in the dark.
Travelling to new places caused anxiety – everyone had experienced getting lost in unfamiliar places and was frightened about this happening again. Everybody was afraid of using public transport at night. We said we felt safer when we had a mobile phone on us, which was switched on and had some credit.
Road safety was also an issue – people were frightened to cross busy roads, which was made worse by the memory of a friend who died in a hit-and-run incident a few years ago.
Everyone wanted more community activities to do, especially in the daytime, such as ten pin bowling and coach trips. People also mentioned unrealised dreams – visiting London, travelling abroad, going to football matches and pop concerts and just having meals out at a pub.
It was important that things should start later in the day so people could use their concessionary bus passes after 9.30am.
Evening activities were also of interest although less so because of the fear of travelling when it was dark.
The chief causes of anxiety creating barriers to community involvement were: going to new places alone; meeting new people; large groups; crowded places; trying to start conversations; getting lost; having to ask for directions; no wi-fi or internet access for map apps; travelling in the rush hour; evening travel; using more than one bus; understanding bus timetables; and frequent changes to bus routes and numbers.
Interestingly, the main barriers are not people being unwelcoming or a lack of money. They are much more about practical issues, such as finding out what is available and help and support so people can start getting involved and travel safely.
This project has shown how we all experience a lot of anxiety and fear, mainly to do with community safety. We have thought about what should change to enable more community inclusion and so help reduce isolation and loneliness.
We will be doing more research over the next year with other people with a learning disability to see if they agree with the barriers that we have identified. Then we need to find out what they think should change so that they and other people with a learning disability can be more included.
The research group comprises eight people with a learning disability in the West Midlands. It is part of Building Bridges Training: www.building-bridges-training.org
Being safe and welcome: what would help
Easy-read information about social and leisure activities, including on how to get there
Advocacy for people with difficult family situations so they can spend their own money on community activities
Support to go to community places for the first few times
Opportunities to do things with support where we don’t have the skills to arrange it ourselves, such as going to concerts or for meals in a pub
Places in the community should be more welcoming
Making staff at sports and leisure venue more aware of the different people in their community who might need support to use the facilities
Better understanding of “invisible disability”, helped by training sessions delivered by people with a learning disability
Using stickers to identify safe places where people with a learning disability who have problems or are scared can go and receive a welcome and practical help

 A dog’s story helps to explain how to recognise, deal with and prevent difficulties when using the toilet, explain a group of reviewers with learning disabilities
A dog’s story helps to explain how to recognise, deal with and prevent difficulties when using the toilet, explain a group of reviewers with learning disabilities