The long-delayed Mazars review is out today (see here Mazar’s Report). For those of you unfamiliar with the Mazars review, this is a review of all deaths of people with learning disabilities and people with mental health problems in Southern Health NHS Foundation Trust services over a four-year period, from April 2011 to March 2015. After meeting @sarasiobhan, one of David Nicholson’s last acts as CEO of NHS England was to commission this review, to find out how many people had died as Southern Health patients and (given Southern Health’s attempt to categorise LB’s death as due to ‘natural causes’ and therefore not requiring an inquest) how Southern Health had investigated (or not) and done something about (or not) their services in the light of these deaths.
The review has been conducted by Mazars, an international ‘audit, tax and advisory firm’ that on the face of it speaks the kind of corporate language I find impossible to understand (see http://www.mazars.co.uk/ ). Two things about this choice are interesting to me. The first is how far NHS England felt they had to go away from the usual networks of ‘experts’ (including ‘experts’ in supposed ‘independent reviews’) to have a hope of getting a truly independent report that would be less enmeshed in the interpersonal webs of people feeding off the freelance margins of the health service. The second thing is that, in my experience, people and organisations whose job isn’t specifically to ‘support’ people with learning disabilities often behave with far more decency, respect, and straightforward professionalism than supposed ‘specialist’ staff/services. It’s almost as if no-one’s told them that people with learning disabilities are only occasionally and provisionally citizens at all, and they perversely insist on treating people with learning disabilities as just, well, people.
In this blogpost I want to go through some of the findings of the Mazars review, focusing on people with learning disabilities within Southern Health (I’m sure others will focus on the equally shocking set of findings concerning people with mental health problems), and say what I think these findings mean. Up front, can I say that in the ‘modern way’ era of shiny corporate euphemising bullshit, this report reveals a state of affairs that is quite the equal of any institutional era inquiry in its deliberate disregard for human life. I will try and avoid rhetorical excess but I warn you; if you have a scintilla of decency then reading this report will rightly put you in a very bad place.
So, a bit of context about Southern Health NHS Trust. The Mazars review covers a four-year time period, from April 2011 to March 2015. In April 2011 Southern Health Foundation NHS Trust came into being, formed when the specialist (largely mental health and learning disability-focused) Hampshire Partnership NHS Foundation Trust took over NHS primary care services across Hampshire. A further acquisition, of a specialist learning disability trust covering Oxfordshire, Wiltshire and Buckinghamshire (the former Ridgeway Trust) took place in November 2012. The current CEO of Southern Health NHS Foundation Trust, Katrina Percy, started as Chief Executive (designate) for the Hampshire Partnership Trust in May 2007, and has remained Chief Executive until the time of writing this blogpost.
Two reasons for sharing this context: 1) despite Southern Health’s attempts to pin the blame on those pesky rogue staff in runaway Ridgeway, this review covers a substantial period of time before Ridgeway was ‘acquired’. 2) Southern Health has had the same CEO before, throughout and after the period of the review, who has surely been fundamental to shaping the culture and practices of the Trust. And if “The fact is, good leadership leads to better care”, as stated by none other than Katrina Percy (http://www.leadershipacademy.nhs.uk/blog/leadership-when-the-going-gets-tough/ ), then it is surely the corollary that worse care (as LB’s inquest so heartbreakingly demonstrated) is caused by bad leadership.
Expect the unexpected (death)
What did the Mazars review do? Page 7 of the report sets this out clearly. “It is not a clinical case review of each service user and we have therefore not tried to identify clinically avoidable deaths. It does seek to establish the extent of unexpected deaths in Mental Health and Learning Disability services provided by the Trust and to identify any themes, patterns or issues that may need further investigation based on a scope provided by NHS England.” As the Mazars review also says, many people do not die an unexpected death (although expected deaths can still be avoidable, see http://chrishatton.blogspot.co.uk/2015/12/death-star.html ), and reporting/recording/reviewing can be more difficult if a person has been using a specialist NHS service (in the case of Southern Health, this includes community-based support and social care as well as inpatient services) but their place of death is elsewhere, such as an acute hospital. This does not excuse a specialist Trust from its responsibility to make sure that:
• “There are thorough and challenging reviews undertaken when the death of a service user happens unexpectedly – regardless of the location of the death;
• These are not necessarily serious incident investigations but occur in a range of ways including clinically led mortality reviews;
• The learning from national reports is applied when making decisions about local investigations;
• There is an open, transparent and independent approach to investigations with the intention of securing all the evidence needed;
• Families and carers are involved where at all possible;
• Reviewers are trained and investigations are of a high standard;
• Lessons are shared widely between providers, commissioners and other agencies; and
• That organisations investigate incidents of unexpected deaths jointly where appropriate.”
While Southern Health have been fighting a rearguard action against the publication of the Mazars review on the grounds of methodology and briefing in ways that only seem to reveal a horrific misunderstanding of their role, it seems to me that: 1) the Mazars review team has done a painstaking job of picking through the chaos of the reporting systems used by Southern Health and has been appropriately cautious in its conclusions (which makes them all the more damning); 2) Southern Health wouldn’t know a rigorous, unspun methodology if it took the form of Jiminy Cricket and perched, whistling, on their collective shoulders.
What did they find? If you have the stomach for it, it’s really worth reading the report itself (weirdly, the Executive Summary is at the, er, front, which devotees of the Verita 2 report will know is not how it’s done), but here goes…
From April 2011 to March 2015, there were in total 337 deaths of people with learning disabilities who had been using Southern Health learning disability services – this includes 38 people with learning disabilities who were using Southern Health’s social care service, TQ21. That’s over 80 deaths of people with learning disabilities using Southern Health every year, including almost 10 people every year in TQ21 social care services. As well as this horrifying number of deaths, the average age of death of people with learning disabilities using Southern Health services was 56 years – a full 7 years younger than the already shockingly young average age of death reported in CIPOLD. Southern Health hadn’t looked at this, of course, or considered early mortality as an issue worthy of attention.
In addition to the total number of deaths recorded on the now notorious RiO system, Southern Health also recorded any ‘unexpected’ deaths on their Ulysses system (presumably medications are recorded on a Getafix system?). Over the four years, 157 of the 337 deaths (that’s 47%, not far off half of all deaths) were recorded in this system as ‘unexpected’. The Confidential Inquiry into Premature Deaths of People with Learning Disabilities (see CIPOLD final report page 34) defined an ‘unexpected death’ as a “death which was not anticipated as a significant possibility 24 hours before the death or where there was a similarly unexpected collapse leading to or predicating the events which led to death”; they found that 43% of deaths of people with learning disabilities were unexpected.
An unexpected death should be serious stuff, shouldn’t it? If a person using your service dies in a way you wouldn’t have predicted 24 hours before, you’d want to find out why and how, so you can tell the family honestly what happened and do everything you can to make sure it doesn’t happen to other people – wouldn’t you? Not within Southern Health, apparently. Their policy is to complete an Initial Management Assessment (IMA) within 24 hours, which does some preliminary scoping of the circumstances of every unexpected death and help determine whether further investigation is needed. Only 66 of the 157 unexpected deaths reported (42%) even got as far as getting one of these assessments done.
Even worse, the quality of these assessments was often shoddy, to put it mildly, with no clear rationale for why investigations shouldn’t go further, little evidence that directors paid attention to them, no evidence of involvement from family members, and no action plans attached to them. Despite the fact that over half of these IMAs concerned people who had apparently died in an acute hospital, joint investigations with the acute Trust were not carried out.
The Mazars team conducted a review of the content of these IMAs, revealing harrowing stories (similar to CIPOLD) which, if taken seriously, could have prevented further deaths of people with learning disabilities within Southern Health. Common issues emerging from IMAs concerned the identification and management of dysphagia and helping people to eat and drink safely, problems with PEG feeding, and not ensuring people got the hydration and nutrition they needed (my heart goes out to @justicefornico here). Other common issues were the (lack of) liaison with acute hospital learning disability liaison staff, and support workers in residential services being slow to recognise and do anything about signs of deteriorating health.
Surely a good proportion of unexpected deaths would require a Critical Incident Review, another level of internal Southern Health investigation and reporting using Root Cause Analysis (it’s all still internal at this stage, with no reporting to external databases required)? And then, if a death meets certain criteria, the trust has to report it within 48 hours to the national Strategic Executive Information System as a Serious Incident Requiring Investigation (SIRI), which while still conducted internally has to be reported to commissioners.
Let’s have a round of ‘Play Your Cards Very Wrong’ shall we? Of the 157 unexpected deaths of people with learning disabilities (or the 66 where they bothered to do an IMA), how many went forward for a Critical Incident Review or were reported as a Serious Incident Requiring Investigation? Lower, lower, no, still lower, LOWER. Two people’s deaths got as far as a Critical Incident Review and two people’s deaths were recorded as SIRIs. In total, 99% of unexpected deaths of people with learning disabilities were not recorded on a national system that would have brought them to the attention of commissioners or the CQC.
When commissioners did get the SIRI reports, they often complained of delays, had to return them because they were of such poor quality, or had to reopen investigations ‘closed’ by the Trust. Of course, commissioners also showed few signs of actively pressing for complete and better information on the deaths of people with learning disabilities, instead supinely accepting the information they were given without wanting to look too closely.
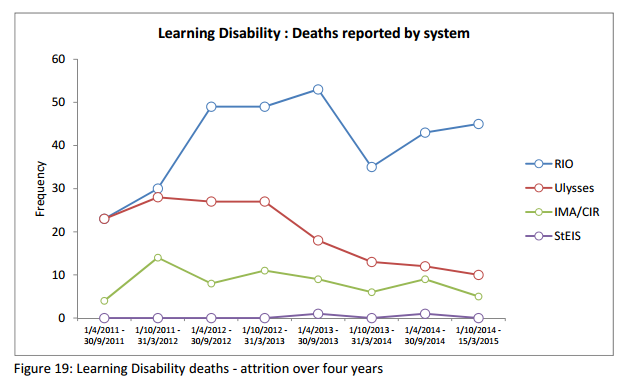
And as for Southern Health’s favourite phrase, learning lessons? What to make of Figure 19 from the Mazars review (I’ve copied this in below – RiO is the reporting of all deaths, Ulysses is the reporting of unexpected deaths, IMA/CIR is deaths where some form of investigation has occurred, and StEIS is deaths reported as SIRIs), showing that, for people with learning disabilities, “the Trust has steadily reported and investigated fewer deaths each year over the period of the review”? Surely a Trust with steady feedback from coroners about their terrible recording and investigation processes around deaths would be getting better at identifying unexpected deaths and investigating them properly? For people with learning disabilities, it would seem the opposite is happening – some form of anti-learning?
I’m bored, I’m the chairman of the board
As someone who has struggled with Southern Health Board papers from time to time, I can only admire the systematic trawl of the Mazars team through a swathe of Board papers. Again, their major conclusions are damning. Only the number of suicides was consistently reported to the Board over time (the rest was subject to ever-changing kaleidoscopic dashboardification), and only unexpected deaths resulting in SIRIs (already winnowed down severely as we’ve seen) rather than all unexpected deaths were reported to the Board.
The Board Assurance Framework makes no mention of unexpected or premature deaths, and the Board papers report constant reassurances from executive directors about the robustness of the SIRI investigation process without any supporting evidence. Again, despite multiple warnings from coroners documented by the Mazars team, there is little evidence that the Board even knew of these warnings, let alone did anything about them. [As an aside, one of the many occasions when a sentence drew an expletive from me was the fairly jaw-dropping fact that Southern Health had been involved in at least 375 mental health or learning disability inquests in the last 4 years – these coroners really need to get their heads together].
In the executive summary, the Mazars team are very clear in detailing the main findings and what follows from them. Rather than repeating it all (do read them – they’re unusually clear) here are a few quotes:
“The failure to bring about sustained improvement in the identification of unexpected death and in the quality and timeliness of reports into those deaths is a failure of leadership and of governance.”
“In our view there has been a lack of leadership, focus and sufficient time spent on reporting and investigating unexpected deaths of Mental Health and Learning Disability service users at all levels of the Trust including at the Trust Board. Due to a lack of strategic focus relating to mortality and to the relatively small numbers of deaths in comparison with total reported safety incidents this has resulted in deaths having little prominence at Board level. The systems in place provide no evidence that the Trust has fully reported or investigated unexpected deaths or taken remedial action where appropriate. This is also evidenced by the inconsistent and incomplete nature of the data supplied.”
“Despite the Board being informed on a number of occasions, including in representation from Coroners, that the quality of the SIRI reporting processes and standard of investigation was inadequate no effective action was taken to improve investigations during the review period.”
The heart of darkness
So, how can I try and sum up the Mazars review? Southern Health NHS Foundation Trust, under the consistent leadership of a single CEO (and a core group of Executive and Non-Executive Directors), put in place and maintained a system of recording, reporting and investigating deaths that: 1) had too many ‘filtering’ layers; 2) was unclear; 3) was implemented in a chaotic and incomplete way; and 4) was not scrutinised by the Board at all. The consequence of this ‘system’ was that a high number of deaths of people with learning disabilities, and a high number of unexpected deaths, translated into almost zero investigations that would involve any visibility to the Board, to commissioners, or to the CQC. Despite repeated complaints/warnings from coroners and others about this system, over the four years of the review fewer and fewer deaths were recorded as unexpected or subject to even the most scant level of investigation.
Four thoughts.
First, this is Mid Staffs type stuff, isn’t it? I don’t see how a Chief Executive and a Board with such a record can possibly continue in post.
Second, is Southern Health unusual, both in the rate of deaths of people with learning disabilities (remember CIPOLD also had many more deaths reported to them than they were predicting) and in their reporting practices? The ‘outlier’ argument beloved of Southern Health is irrelevant – if crap smells the same as other crap, it’s still crap. If NHS England really wanted to get to the bottom of this they would give the new national mortality review function run by the University of Bristol (see http://www.bristol.ac.uk/sps/leder/ ) much sharper teeth – mandatory not voluntary mortality reporting, and stricter standards and external scrutiny of the way mortality reviews are done (including how unexpected deaths are defined and reported).
Third, the written statement delivered by Jeremy Hunt for the Department of Health (see here http://www.parliament.uk/business/publications/written-questions-answers-statements/written-statement/Commons/2015-12-17/HCWS421/ ), the joint NHS Improvement (formerly partly Monitor)/NHS England/Care Quality Commission statement (‘leaked’ to me – so sue me), the statement from the commissioners (who they? See Commissioners response to the Mazar’s report) reveal a comprehensive failure on a scale that is insulting, really. This was an acid test of whether, for all the signed #changeday light bulbs, cascading workstreams, fine words about the 6Cs [add no, no, in, mis, no, and no to this list and you’re about there https://www.england.nhs.uk/wp-content/uploads/2012/12/6c-a5-leaflet.pdf ], and endless plans re-spun in the wake of nothing happening, these organisations were going to stand together with people with learning disabilities and families when the chips were down. A test which has been monumentally flunked:
• The delay and two fingers symbolism of the timing of the reports publication, and the written statements.
• The complete lack of recognition that accountability is required for what has happened at Southern Health and the lack even of a mention that what occurred might be, erm, bad (the CQC will do ANOTHER focused inspection – there have been many of Southern Health, which have been damning in what they’ve found in their services for people with learning disabilities – oh, and then they’ll chat to the invisible Monitor, where no doubt there will be agreement that ‘progress has been made’ and, er, that’s it).
• The sliding elision from Southern Health responsibility to airy questions of general culture – yes, absolutely this may be happening elsewhere, but what message does letting Southern Health off the comfy velvet hook of supposed monitoring send?
• Despite the repeated, repeated, repeated evidence from people who have actually engaged with Southern Health over the years of how they roll, a bland (and by now knowing) public acceptance that it was a small error of paperwork which they’re sorting out now it’s been brought to their attention. If I get pissed and assault someone, I’m sure the police will be very understanding the next morning when I explain that I’ve taken measures to mitigate my drunken violence by sobering up overnight in the police cell, so there’s no need to charge me with anything is there?
• The bland phrases that trip off the apparatchik’s tongue: “the report is critical”; “there is more to do”; “we agree with the spirit of this recommendation”. This is perfectly encapsulated in a video clip Jeremy Hunt has circulated on his twitter feed, where you can see/hear him saying “Whatever may or may not have gone wrong” (yes, really).
• The reassurance that the CCGs will hold Southern Health to account, despite the fact that they have repeatedly shown no will or capacity to do this so far.
In both responses, I can see the traces of the usual civil service innovo-whip-round. What are we already doing that we can dress up as a new initiative that’s responding to what’s happened? Writing a note to Medical Directors offering help? Pur-lease, as my daughter says. The national mortality review function already exists, and these statements say nothing about beefing up its powers in the light of what Mazars have reported (for services, participation is voluntary, for example). They say they will try and collect better information about services, which is something that is already part of the Transforming Care programme.
I know there are excellent people working in NHS England and the Department of Health who are highly committed to improving the lot of people with learning disabilities and their families (if you are reading this, I’m hoping you will know who you are) and they are good people trying to do good things in difficult circumstances who I respect greatly. But what does this say about the capacity of these organisations to really stand shoulder to shoulder with people with learning disabilities and families? After this, why should a whole bunch of people trust organisations that, when it comes down to it, can’t deliver? If they can’t address the implications of the Mazars report properly, how on earth are they going to ‘Transform Care’ with their ‘Big Plans’ and ‘Service Models’. Ask yourself, who is anxious and who is reassured tonight?
Finally, for me the Mazars review brings into the open what feels like a fundamental disregard for the lives of people with learning disabilities, even within organisations that are supposed to be supporting people. We can’t pussyfoot around any more with more guidance but only if you feel like it, more soft-soap persuading people to do the ‘right thing rather than the wrong thing’ (why are people doing the wrong thing still in their jobs?). We need to confront this head on, cut the crap and say the thing itself. At least we now know that we can’t rely on the Department of Health, NHS England or the accountability roundabout. More and more I think the only way to really cut through the miasma of quietude is to really, really, put people with learning disabilities and families in charge.
Six hours’ silence
Right at the start of the Mazars review report, the Acknowledgements section begins with this:
“This report presents a lot of numbers. The team recognise that each number represents a loved one and would like to give their condolences to the families of every person referred to in the following chapters.”
337 lives, all different, all irreplaceable. If we held a minute’s silence for each of the 337 people with learning disabilities who died, we would be silent for almost six hours (and this is just one NHS Trust). And once this period of silence is over (as we have seen, there is too much silence, too many whisperings behind closed doors) we must not, cannot, return to business as usual. Business as usual is killing people [and there’s the rhetorical excess…]


